Rabies Consent
advertisement

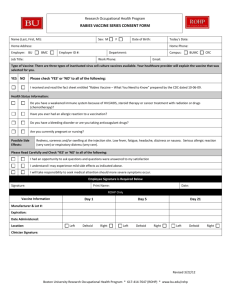
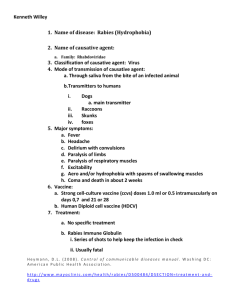
Rabies Vaccine Consent From What is Rabies? Rabies is a virus which causes an acute infectious disease in mammals. It is often present in the saliva of infected (rabid) animals. The disease is transmitted by a rabid animal biting another animal/human, or by exposure to the infected animal’s saliva on an open wound or mucous membrane. The incubation period is 10 days to one year. Usually, symptoms begin between 30 to 50 days following exposure. The virus affects nervous tissue in humans. Common initial symptoms are restlessness, tiredness and fever. As the disease progresses, symptoms of uncontrollable excitement with excessive salivation and painful laryngeal/pharyngeal spasms can occur. Indications The vaccine is indicated for veterinarians, some laboratory workers and animal handlers. Dosage The Rabies vaccine is given in three doses at the following intervals: Initial dose Second dose given one week later Third dose given 21 to 28 days following the initial dose The vaccine is proven effective for up to two years. It is recommended that immunity status be checked every two years and booster doses be given if indicated. Possible side effects of the vaccine The most common side effects of the vaccine are soreness, swelling and pain at the site of injection. As with any vaccine, there is a slight chance of allergic or more serious reactions. Consent I have read the above information and had it explained to me. I have had the opportunity to ask questions. I believe I understand the benefits and risks of the rabies vaccine. I give consent that the rabies vaccine be given to me as part of my treatment. Patient Signature _____________________________________________ Date ____/____/____ Witness Signature ______________________________________________ Date ____/____/____ Declination I have read the above consent and understand the risks and benefits of the vaccine and decline the vaccine at this time. Patient Signature _____________________________________________ Date ____/____/____ Witness Signature ______________________________________________ Date ____/____/____ If you decline the vaccine, please indicate your reason ______________________________________ __________________________________________________________________________________ Rabies Vaccine Consent Form Patient Name ________________________________________________ Date _____/______/______ Vaccination status □ Never vaccinated □ Vaccinated no documentation □ Vaccinated more than two years ago Pre-testing blood work: (Rabies Endpoint Titer) Date Drawn _____/_____/_____ Results: □ Immune □ Susceptible Rabies vaccination series 1. 1 ml IM □ Left Deltoid □ Right Deltoid Date ____/____/____ Lot # _________________ Nurses Signature ________________________________________ 2. 1 ml IM □ Left Deltoid □ Right Deltoid Date ____/____/____ Lot # _________________ Nurses Signature ________________________________________ 3. 1 ml IM □ Left Deltoid □ Right Deltoid Date ____/____/____ Lot # _________________ Nurses Signature _______________________________________ Post vaccination blood work Date due: _____/_____/_____ Date done: _____/_____/_____ Results: □ Immune □ Susceptible Rabies boosters 1. 1 ml IM □ Left Deltoid □ Right Deltoid Date ____/____/____ Lot # _________________ Nurses Signature ________________________________________ 2. 1 ml IM □ Left Deltoid □ Right Deltoid Date ____/____/____ Lot # _________________ Nurses Signature ________________________________________ 3. 1 ml IM □ Left Deltoid □ Right Deltoid Date ____/____/____ Lot # _________________ Nurses Signature ________________________________________ Please mark your calendar as a reminder for vaccination and follow-up as scheduled. This form also serves as a record of your vaccination.