Cosmetic Reconstructive Services Skin Related
advertisement

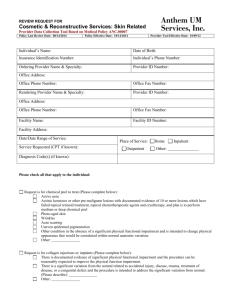
REVIEW REQUEST FOR Cosmetic & Reconstructive Services: Skin Related Provider Data Collection Tool Based on Medical Policy ANC.00007 Policy Last Review Date: 02/26/09 Policy Effective Date: 02/26/09 Provider Tool Effective Date: 10/01/09 Member Name: Date of Birth: Insurance Identification Number: Member Phone Number: Ordering Provider Name & Specialty: Provider ID Number: Office Address: Office Phone Number: Office Fax Number: Rendering Provider Name & Specialty: Provider ID Number: Office Address: Office Phone Number: Office Fax Number: Facility Name: Facility ID Number: Facility Address: Date/Date Range of Service: Service Requested (CPT if known): Place of Service: Outpatient Home Inpatient Other: Diagnosis (ICD-9) if known): Please check all that apply to the member: Request is for any of the following: Treatment of Telangiectasias Temporary or permanent renmoval of hair for hirsutism Hairplasty for male pattern alopecia Removal or excision of a tattoo. Request is for Chemical peel—[epidermal peels or chemotherapy of the skin] (Please complete below): Member has active acne To treat photo-aged skin, wrinkles, acne scarring or uneven epidermal pigmentation Other: Request is for medium or deep Chemical peel—[dermal peel] (Please complete below): Documented evidence of 10 or more actinic keratoses or other pre-malignant lesions Member has failed topical retinoid treatment, topical chemotherapeutic agents and cryotherapy To treat photo-aged skin, wrinkles, acne, acne scarring or uneven epidermal pigmentation Other: Request is for Collagen Injections or Implants (Please complete below): Documented physical functional impairment & the treatment can be reasonably expected to improve the physical function impairment. Need for restoration and there is significant variation from the normal related to accidental injury, trauma, treatment of disease, or congenital defect. (Please describe): ______________________________ Other: Request is for Dermabrasion or Salabrasion (Please complete below): Documented evidence of the removal of 10 or more superficial basal cell carcinomas and precancerous actinic keratoses Member has failed topical retinoid treatment, topical chemotherapeutic agents and cryotherapy For abrasion of the upper layer of the skin for acne, acne scars, uneven pigmentation or wrinkles Other: Request is for laser and surgical treatment of Acne Rosacea (Please complete below): The member has severe and refractory form of Rosacea unresponsive to standard medical therapy. The member has had an adequate trial of topical or oral agents or both (antibiotics). There is documentation that the individual has undergone and received inadequate results with conservative management Preoperative photos document the clinical skin changes requiring treatment *** Please attach photo’s. Other: Request is to treat permanent telangiectasia (Please complete below): Using electrosurgery Using laser (pulsed dye V-beam, the 585 flash pump laser, KTPlaser) Using intense pulsed light (IPL) therapy Other: Request is to treat severe rhinophyma (Please complete below): Using radiofrequency cutting current and a hockey puck adapter Using carbon dioxide laser peel Using surgical shaving Other: Request is for treatment of keloids (Please complete below): Documented physical functional impairment related to the keloid & the treatment can be reasonably expected to improve the physical function impairment. Keloids themselves produce significant anatomic variance Other: Request is for Scar Revision (Please complete below): There is documentation of physical functional impairment related to the scar the treatment can be reasonably expected to improve the physical function impairment. Need for restoration and there is significant variation from the normal related to accidental injury, disease, trauma, treatment of disease, or congenital defect. (Please describe): ______________________________ Other: Request is for Tattooing of the skin (Please complete below): Done as part of a medically necessary therapeutic process (ie, radiation therapy, or as a result of reconstructive Breast surgery. Other: Request is for the injection of dermal fillers, such as poly-L-lactic acid (Sculptra), and a synthetic calcium hydroxylapatitie (Radiesse) when used to address a significant variation from normal (Please complete below): Realted to accidental injury Related to disease or trauma For the treatment of a disease or congenital defect Other: Request is for the treatment of port wine stain with laser or other methods (Please complete below): To restore appearance when used to address a significant variation from the normal related to a congenital defect Other: Other: Page 2 of 3 This request is being submitted: Pre-Claim Post–Claim. If checked, please attach the claim or indicate the claim number By checking this box, I attest the information provided is true and accurate to the best of my knowledge. I understand that Anthem may perform a routine audit and request the medical documentation to verify the accuracy of the information reported on this form. _____________________________________________________________ Name and Title of Provider or Provider Representative Completing Form (Please Print)* Date *The attestation fields must be completed by a provider or provider representative in order for the tool to be accepted Services provided by Empire HealthChoice HMO, Inc. and/or Empire HealthChoice Assurance, Inc., licensees of the Blue Cross and Blue Shield Association, an association of independent Blue Cross and Blue Shield plans. For some plans utilization review services are provided by Anthem UM Services, Inc., a separate company. Page 3 of 3