Cases and Questions - Stritch School of Medicine
advertisement

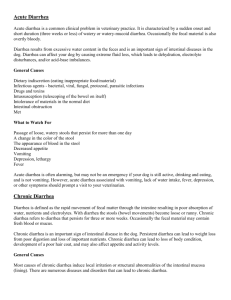
CONTINUITY CLINIC CURRICULUM CHRONIC DIARRHEA GOALS AND OBJECTIVES: 1. Be able to discuss both the common and more rare causes of chronic diarrhea and understand the natural history of the multiple sub-types of chronic diarrhea. 2. Be able to utilize a systematic diagnostic and cost effective approach in the evaluation of chronic diarrhea based on the current recommendations. CASE STUDY 1: A phone message is handed to you at Noon on Friday: Ms S. called, she wants to talk to you about the diarrhea she has been having On review of her chart you note that she is a 23 year old, who saw you 5 weeks ago for a UTI and was treated with Amoxicilin for seven days.. She had also just returned from a camping trip to Colorado. She had no risk factors for HIV, and has a family history of "colitis" from her maternal grandmother. 1. Given the above information, what is relevant in her chart and what questions should you ask the patient over the phone in an attempt to decide whether she will come in this afternoon (in your last acute appointment spot) or can be reassured and an appointment scheduled for Monday. She states that she has had diarrhea for 4 two 5 weeks now, however, she had prior episodes which lasted only for a week or so. She relates some improvement with fasting, but not resolution and has had nocturnal symptoms. She denies the presence of blood or mucous, and states the bowel movements are less formed, but not frothy or difficult to flush. Upon further questioning, she says while hiking she only drank purified water. 2. Given the above information, when will you see the patient, and if not today what advise would you ask the patient to follow until her appointment. Please include in your telephone documentation which symptoms and signs altered your management. At the office, the patient reports no improvement while following your advise. She restates the above history and elaborates that this has happened two the three times a year since her teens. Each episode has been self limited, and associated with weight loss, but no identifiable life stresses. Medications: none currently including over the counter drugs, Amoxicilin 6 weeks ago Physical Examination: Height 5'4" weight 118 lbs. (down 9 lbs. over 6 weeks) Afebrile 110/65 68 14 not orthostatic HEENT: pale conjunctiva, oral membranes moist Neck: non palpable thyroid Lungs: Clear Heart: regular rhythm normal s1 and s2 Abdomen: soft non tender or distended, normoactive bowel sounds, no masses No organomegaly, no guarding Rectal: guiac positive, brown stool 3. How does this information affect your differential diagnosis and which laboratory studies, radiologic studies and endoscopic studies may be warranted, and in which order. Laboratory values include WBC 8.0 HgB 9.0 Pts 146 MCV 72, electrolytes, bun, creatinine all normal, ESR 55, fecal WBC + and fecal RBC +. Ova and Parasites negative and C. diff toxin negative. 4. What further work up would you peruse at this point? A colonoscopy was performed and multiple biopsies taken which were read as normal. An EGD was also performed and biopsies revealed flattened villi and leukocytic infiltration. An anti-gliadin antibody was also ordered and returned positive. 5. What is the diagnosis and the appropriate therapy. CASE STUDY 2: A 50 year old female presents to your office as a new patient, having moved to the area. She has a past medical history of irritable bowel syndrome since her teens and B12 deficiency for five years. She denies any history of thyroid disease or diabetes. She does have osteoarthritis of the knees which limit her activity. She reports a worsening of her diarrhea over the past two years with an associated twenty pound weight loss. The stool is loose in character and she states floats in the bowel and is very foul smelling. She also has new onset of nocturnal diarrhea over the last year, but notes no blood or mucous, change in stool color or caliber. Family History: no cancer, no colon diseases Social History: quit tobacco 25 years ago, rare ETOH, no laxative use Dietary History: 2-3 cups of coffee per day, 1 glass of milk Attempted lactose and gluten free diets on her own without success Medication: prior use of loperamide Cyanocobalamine injections q Month Physical Examination: Mildly obese female, appears states age. Afebrile 78 138/84 14 HEENT: unremarkable Neck: no masses, non palpable thyroid Lungs: clear Heart: regular rhythm, normal s1s2 no murmurs Abdomen: soft, non tender or distended, no masses Rectal: brown, guiac negative Extremities: crepitance of both knees with minimal deformity Recent laboratory values ESR 14 WBC 11.5 HgB 13 Pts 164 Eos 7% 98 Stool O and P negative, Giardia antigen negative, Stool WBC + and RBC 1. MCV From the information given, what etiologies for the patient symptoms would you consider, and what further studies would you obtain? A stool gap was <50, and the patient was unable to collect a 72 hour fecal fat collection secondary to limitation from her osteoarthritis. 2. How would you interpret this information, and what point should a patient be admitted to the hospital for further workup? 3. What is your differential diagnosis and what studies will aid in determining the etiology? Colonoscopy was grossly normal, however, multiple biopsies revealed a lymphocytic infiltrate with prominent collagen bands. 4. What diagnosis does this suggest, and what is the appropriate therapy? PLEASE FILL OUT THE EVALUATION FORM, TEAR IT OUT AND PLACE IT IN THE APPROPRIATE CLINIC DROP OFF LOCATION. BIBLIOGRAPHY: *1. AGA guideline: Evaluation and management of chronic diarrhea. 2. Bayless TM. Chronic diarrhea, newly appreciated syndromes. 1989:117-135. Hosp Pract. Jan DiJohn D, Levine MM. Treatment of diarrhea. Infect Dis Clin North Am. 1988;2:719-745. *4. Donowitz M, Kokke FT, Siadi R. Evaluation of Patients with Chronic Diarrhea. NJEM. 1995;332:725-729. 5. Lipsky MS, Adelman M. Chronic diarrhea: Evaluation and treatment. Am Fam Physician. 1993;48:1461-1466. 6. Longstreth GF. Irritable Bowel Syndrome: Diagnosis in the Managed Care Era. Digestive Diseases and Sciences. 1997;42(6):1105-1111. Lynn RB, Friedman LS. Irritable Bowel Slyndrome. NJEM. 1993;329:1940-1945. 8. Powell DW. Approach to the Patient with Chronic Diarrhea. Yamada T ed. Textbook of Gastroenteroloty Phyiladelphia. JB Lipincott 1995. Tatal AH, Murray JA. Acute and chronic diarrhea. How to keep laboratory testing to a minimum. Postgraduate Medicine. 1994;96(3):30-32, 35-38, 43. *Required reading