5_6 2-3 (Schafer)
advertisement
")
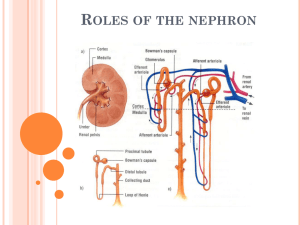
Renal: 2:00 - 3:00 Scribe: Chaz Capra Wednesday, May 6, 2009 Proof: Teresa Kilborn Dr. Schafer Regulation and Measurement of GFR Page 1 of 4 I. Renal physiology – Lecture #3 [S1]: a. Filtration, reabsorption, and secretion as determinants of excretion b. The clearance concept c. How we use clearance to measure glomerular filtration rate (GFR) and renal plasma flow (RPF) d. Operation of nephron segment, the proximal tubule e. Reabsorption of 2/3 of the filtered solute and water f. Tm-limited reabsorption II. Mass balance along the nephron [S2] a. filtration stays constant most of the time b. we determine what is excreted by regulating the rate of reabsorption and the rate of excretion c. excretion rate = [rate of filtration] – [rate of reabsorption] + [rate of secretion] i. reabsorption is taking substances from nephron and returning it to the blood ii. secretion is taking substances from the blood and secreting it into the nephron III. Solute movements between nephrons and capillaries [S3] a. 120 – 130 mL/min is being filtered i. the filtered substance is an ultrafiltrate (meaning protein free) b. most of this fluid is reabsorbed (actively transported across the epithelium of the nephron to the blood) into the peritubular capillaries; therefore, it is being returned to circulation as if it were taking a detour c. Substances that are secreted are potential toxins or drugs i. secretion is usually at low rate, except potassium (K+) which has a high rate ii. most secreted substances are organic solutes iii. active processes across the nephron, particularly the proximal tubule, that put the substance into the urine; this will increase the urinary excretion rate of that substance + IV. Example of Na reabsorption [S4] a. He mentioned that he doesn’t want us to memorize the numbers on this slide, nor will he expect us to calculate filtered load, reabsorption, or excretion; the purpose of the slide is to get an idea of quantity. It shows a comparison of the relative amounts of Na+ that are filtered, reabsorbed, and then excreted b. The amount of sodium can be calculated by multiplying the GFR by the plasma concentration of sodium i. normal GFR = 180 L/day c. The amount of sodium you excrete depends on how much salt you ingest in your diet i. excretion can be calculated by multiplying urine flow (rate of urine production) by the concentration of sodium in the urine d. There is a large difference between the amount of sodium filtered and the amount that is excreted; this is due to sodium reabsorption i. it is vitally important to regulate how much sodium the body excretes; this is to help maintain a daily salt balance (the body regulates how much is excreted to match the dietary intake) 1. if you retain too much salt, you get thirsty 2. this leads to salt and water retention which can progress to edema in your ankles, face, hands, etc. ii. the amount that is excreted is regulated by reabsorption 1. over 99% of what is filtered is reabsorbed V. The clearance concept [S5] a. Clearance: this is one way of expressing the kidney’s function to eliminate a substance from the body through excretion in the urine i. the clearance of a solute represents the volume of plasma that is “cleared” of that solute per minute ii. this is an abstract concept: the kidneys are operating by excreting substances to clear plasma of that substance; it is expressed as mL/min 1. the higher the clearance rate, the more effectively the kidneys are getting rid of that substance b. How well is a kidney excreting a substance “X”? i. this can be determined by the product of the concentration of “X” in the urine and the urine flow rate (UF) c. How well are you excreting substance “X” relative to its concentration in the plasma? i. calculated by normalizing the excretion rate with plasma concentration of “X” ii. this gives you the clearance (Cx) of that substance: excretion rate divided by the plasma concentration = Cx VI. Rate of inulin excretion = rate of filtration [S6] a. He says that memorizing these numbers is not important b. Inulin doesn’t normally appear in the body i. it is a polyfructose starch Renal: 2:00 - 3:00 Scribe: Chaz Capra Wednesday, May 6, 2009 Proof: Teresa Kilborn Dr. Schafer Regulation and Measurement of GFR Page 2 of 4 ii. inulin is a useful aid for renal physiologists to measure GFR, because it is inert; meaning that it is not reabsorbed and not secreted, but it is freely filtered into the nephron c. To measure inulin clearance in an individual, you have to infuse it intravenously; therefore, it is only useful in a research setting (he uses it to illustrate a principle to us) d. Calculating the filtration rate of inulin: (GFR) 130ml/min multiplied by (plasma concentration) 1mg/dl = 1.3mg/min of inulin filtered into the nephron e. The big advantage of inulin: it can’t be reabsorbed (due to its large size) nor is it secreted; this means that everything that is filtered is going to be excreted i. therefore, the rate of excretion is equal to the rate of filtration (GFR = Excretion rate) f. Calculating the excretion rate: urine flow (UF) 1ml/min multiplied by the (urine concentration of inulin) 130mg/dl = 1.3 mg/min i. notice the urine concentration of inulin is larger than the plasma concentration; this is due to the reabsorption of the water out of the tubule and into the blood VII. The clearance of inulin is equal to the GFR [S7] a. The real advantage of inulin is that it’s clearance rate is equal to the GFR; inulin is used to determine the filtration rate of the kidney i. all the inulin that is in the plasma gets filtered, and all the inulin that gets filtered is excreted VIII. Clinical estimation of GFR from creatinine clearance or plasma creatinine concentration [S8] a. Creatinine is endogenous (produced in the body); it is the best indicator of GFR clinically i. it is a byproduct of metabolism and its elimination from the body is necessary 1. it is a byproduct of the breakdown of creatine phosphate in muscle 2. it has a high daily production that is constant for a given individual; people who work out frequently will have a higher rate of creatinine production b. Creatinine comes as close to inulin as you can get i. it is freely filtered, it is not reabsorbed, and it is secreted but in very small amounts (contributes less than 10% to the total excretion); therefore, we make the assumption that creatinine is neither reabsorbed nor secreted ii. the amount of creatinine excreted daily needs to remain constant with and approximately equal to the amount that is produced daily 1. UF X Urine concentration (creatinine excretion) is approximately equal to GFR X plasma concentration (creatinine filtration) 2. creatine excretion is a little bit more than its filtration (due to the small amount that is secreted), so this means that creatinine clearance is going to overestimate the GFR a little bit a. however, making the assumption that creatinine is not secreted makes creatinine clearance a good indicator for GFR c. A measurement of GFR can be done clinically; it is usually done in patients who have chronic kidney disease i. in kidney disease, there is destruction and scarring in the vessels due to inflammatory processes 1. Nephrons are lost as the disease progresses leading to a falling GFR; therefore, falling GFR is a marker of kidney disease 2. creatinine clearance is monitored by clinicians to determine the efficiency and health of the kidneys ii. How is creatinine clearance measured? 1. the patient collects his/her urine over a 24 period 2. the volume of the urine is measured and used to calculate urine flow rate 3. calculate the creatinine concentration in the urine, and you take a plasma sample to measure the plasma creatinine concentration 4. from these values, you calculate the creatinine clearance which will be equal to the GFR d. Another good indicator of the progression of the disease is the plasma concentration of creatinine i. How is this a good indicator? 1. the rate of creatinine production is nearly constant, and this means that creatinine excretion rate is nearly constant; therefore, the GFR is inversely proportional to the creatinine plasma concentration ii. Now referring to the graph at the right of the slide 1. normal GFR (x-axis) is 120-130 ml/min & the plasma creatinine concentration (y-axis) is normally 0.5-1 mg/dl 2. as the GFR decreases the plasma creatinine concentration rises exponentially a. measuring the plasma concentration gives a good indicator of GFR; it is a good screen for normal, healthy individuals e. A reduction in GFR becomes clinically important when GFR decreases below half the normal rate (~65ml/min) i. most people can get along fine with just half the normal GFR Renal: 2:00 - 3:00 Scribe: Chaz Capra Wednesday, May 6, 2009 Proof: Teresa Kilborn Dr. Schafer Regulation and Measurement of GFR Page 3 of 4 ii. when GFR becomes critical, it will be necessary for the patient to restrict their diet and closely monitor salt and protein intake iii. end stage renal disease is reached once the GFR drops to 20ml/min or less 1. kidneys have lost ability to maintain homeostasis at this point 2. patient will need hemodialysis or a transplant IX. Example of para-aminohippurate (PAH) secretion [S9] a. PAH is not a normal product of human metabolism, so it has to be infused (like inulin) i. it is very actively secreted (unlike inulin), so that all is removed from renal blood and secreted into the nephron ii. not much of it is filtered in the glomerulus b. Notice that the amount of PAH excreted is about 5 times greater than the amount that is filtered i. this is due to the active secretion of PAH that takes place in the proximal tubule X. PAH as a marker for RPF [S10] a. Due to PAH qualities described in the previous slide, it can be used as a marker for renal plasma flow (RPF) i. the PAH that flows into the kidney is equal to the renal plasma concentration of PAH times the RPF ii. all of the PAH that is in the plasma is excreted (1st equation); therefore, the clearance of PAH is equal to the RPF (2nd equation) XI. Key points – lecture #3 (part 1) [S11] a. Mass balance in the nephron: urinary excretion = rate of filtration - rate of reabsorption + rate of secretion b. Renal clearance c. Inulin - neither secreted or reabsorbed: clearance = GFR d. Creatinine clearance as an approximation of GFR. Dependence of plasma creatinine concentration on GFR. e. PAH totally cleared by filtration + secretion: clearance equals the RPF XII. Costanzo figure 6-3 [S12] a. this figure is just to help you get oriented with the different portions of the nephron that will be discussed in detail during future lectures; today’s focus is on the proximal tubule b. pay attention to the order in which urine flows through the nephron from the glomerulus, to the proximal convoluted tubule, to the loop of henle, to the collecting duct XIII. Components of an epithelial cell layer [S13] a. Structure of the epithelial cell layer all along the nephron i. the wall is 1 cell layer thick, and adjacent cells are connected by junctional complexes ii. (in the figure) the urine borders the cells on the left at the lumenal membrane of the cell; the basolateral membrane of the cell borders the basement membrane to the right iii. the peritubular capillaries (not shown) would be located right next to the basement membrane on the right side, so there is very little interstitial space in the kidney XIV. General mechanism of Na+ reabsorption [S14] a. This process of sodium reabsorption is occurring in almost every cell in the nephron (except in the thin descending limb of the loop of henle i. sodium reabsorption is involved in the reabsorption of many other substances b. The general mechanism by which sodium reabsorption occurs: i. sodium enters the cells passively from the lumen, and it is going downhill (it is following the electrochemical gradient); there is less sodium inside the cell & the inside of the cell is more negative ii. differences among nephron segments occur at the type of sodium transporter, but the overall process is the same in all the segments iii. sodium is actively pumped out of the cell via a Na/K ATPase pump iv. potassium is actively pumped into the cell via this pump, and it is circulated out of the cell through the basolateral membrane XV. “Isosmotic” volume reabsorption by the proximal tubule [S15] a. Isosmotic volume reabsorption is the main process occurring in the proximal tubule i. 2/3rds of the water and salt that is filtered gets reabsorbed in the proximal tubule ii. it is called “isosmotic” because the osmolality of the tubular fluid stays the same as that of the plasma; this is due to equivalent amounts of solutes and water that are absorbed; otherwise, the tubular fluid would become diluted or concentrated b. How is water reabsorption being driven? Renal: 2:00 - 3:00 Scribe: Chaz Capra Wednesday, May 6, 2009 Proof: Teresa Kilborn Dr. Schafer Regulation and Measurement of GFR Page 4 of 4 i. sodium is being actively reabsorbed, bicarbonate is actively reabsorbed, chloride is passively reabsorbed, and substances that are metabolically useful (like glucose and amino acids) are also actively reabsorbed; water goes along with the solutes that are being reabsorbed ii. this requires a very high water permeability 1. aquaporin-1 are water channels located in the lumenal and basolateral membranes that provide this high permeability 2. in addition, the proximal tubule is leaky because the junctional complexes between cells are permeable to water, urea, and chloride XVI. Cellular mechanism of glucose reabsorption [S16] a. Glucose is very well absorbed in the proximal tubule by a secondary active transport mechanism i. it is coupled to the reabsorption of sodium to drive the entry of glucose against its concentration gradient (glucose is moving uphill because it is using the energy derived from sodium moving downhill) ii. there is a facilitated transporter on the basolateral membrane that allows glucose to leak out of the cell and back into the blood iii. ultimately, the energy for this secondary active process is created via the action of the Na/K ATPase producing the electrochemical gradient that promotes sodium reabsorption b. the amount of glucose that can be reabsorbed is limited by the number of facilitated transporters present i. if all the transporters are saturated with glucose, any excess glucose will be excreted in the urine XVII. Glucose titration curve [S17] a. If you raise a person’s plasma glucose concentration 2 times above normal, you reach a plasma threshold i. at this point, glucose starts to be excreted in the urine ii. the reason is that some of the nephrons are saturated and cannot absorb anymore glucose b. If the plasma glucose levels elevate further, a transport maximum (Tm) is reached i. at this point the amount of glucose excreted parallels the amount that is filtered XVIII. Reabsorption by Tm-limited systems [S18] a. These systems involve the cotransport of sodium driving substrates into the cell b. This increases its concentration inside the cell c. The substrate is then transported across the basolateral membrane by a facilitated transporter d. The types of substrates that are reabsorbed by the mechanism are glucose, amino acids, lactate, pyruvate, di-& tricarboxylic acids, phosphate, and sulfate XIX. Key points – lecture #3 (part II) Proximal tubule [S19] a. Organization of epithelia b. General mechanism of Na+ reabsorption that occurs all along the nephron c. Na+ reabsorption in the proximal tubule - linked to other solutes and provides energy for their reabsorption or secretion d. Two-thirds of the filtered salt and water are reabsorbed isosmotically - tubular fluid becomes only slightly dilute e. Active reabsorption of many solutes linked to Na+ Glucose as an example of Tm-limited reabsorption [end 46:48 min]