PRISONER TRANSPORT & BOOKING PROCEDURES
advertisement

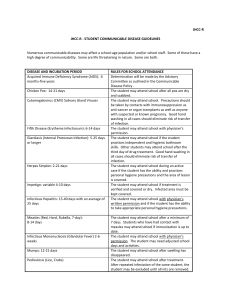
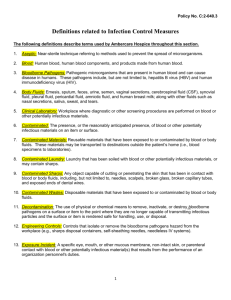
DELAND POLICE DEPARTMENT Chief William E. Ridgway Departmental Standards Directive TITLE: CODIFIED: CFA STD: COMMUNICABLE DISEASE EXPOSURE CONTROL PLAN 4.1 37.01, 37.02, 37.03,37.04, 37.05 DATE OF ISSUE: 01.12.07 EFFECTIVE DATE: 01.12.07 RESCINDS/ AMENDS: PAGES: 04.08.04 10 PURPOSE The purpose of this directive is to provide guidelines for members who are at risk of exposure, in preventing the contraction of communicable disease. POLICY The safe performance of daily operations has recently become threatened by life-endangering communicable diseases. Therefore, it shall be the policy of the department to provide employees with upto-date safety procedures and communicable disease information that will assist in minimizing potential exposure, while increasing their understanding of the nature and potential risks of communicable diseases. DEFINITIONS Exposure Control Plan: A plan of action which is designated to eliminate or minimize members exposure to infectious disease. (Copies of the Exposure Control Plan are assigned to each member as part of their Written Directive Manual). Bodily Fluids: Liquid secretions including blood, semen and vaginal or other secretions that might contain these fluids such as saliva, vomit, urine or feces. 4.1-1 Bloodborne Pathogens are the pathogenic microorganisms that may be present in human blood and/or its components and/or products. Contaminated is the presence or the reasonably anticipated presence of blood or other potentially infectious materials. This may involve laundry, sharps, and equipment. Communicable Disease: Those infectious illnesses that are transmitted through direct or indirect contact with an infected individual. Occupational Exposure (OPIM): Reasonably anticipated skin, eye, mucous membrane, or parenteral contact with blood or other potentially infectious material. Exposure Incident: Contact with a potentially infectious material. This could be parenteral (puncture) and/or percutaneous contact (eye, mouth, other mucus membrane). Exposure Level is the seriousness of an Exposure Incident. Levels of exposure include: Casual Exposure: interaction with a potential source person that does not involve contact with the person’s blood or other body fluids (interviewing, interrogating, conversing, routine arrest). Minimal Exposure: blood or other body fluid from a source person comes in contact with the member’s intact skin; the source person’s intact skin contacts the member’s mucus membrane (blood contacts a member’s intact skin; a combative subject grabs a member’s mouth). Moderate Exposure: blood or body fluid from a source person contacts a member’s mucus membrane (mouth-to-mouth resuscitation; a source person sneezes on a member). Significant Exposure: blood or body fluid from a source person contacts the member’s non-intact skin or open wound, or a percutaneous inoculation, such as a needlestick. Personal Protective Equipment (PPE): Specialized clothing or equipment worn by members for protection against the hazards. This does not include standard issue uniforms and work clothes without special protective qualities. Universal Precautions: Procedures promulgated by the Centers for Disease Control (CDC) that emphasize precautions based on the assumption that all blood and bodily fluids are potentially infectious of the AIDS (HIV) and hepatitis B (HBV) viruses. EXPOSURE DETERMINATION 4.1.1 The Department of Labor, in particular the Occupational Health and Safety Administration has identified a work force which due to the nature of the job function, has a high potential for exposure to bloodborne pathogens, including HIV and HBV. That work force is Law Enforcement, Fire Services, Emergency Medical Services, and Auxiliary Emergency Services. 4.1-2 4.1.2 One of the keys to implementing this Exposure Control Plan is to identify exposure situations personnel may encounter. To facilitate this, the following lists have been compiled: Job classifications in which all personnel have occupational exposure to bloodborne pathogens. All Department sworn police officers, Community Service Aides, and Evidence Technicians could reasonably be anticipated to have occupational exposure to bloodborne pathogens as the result of performing their job duties. Body areas such as face/skin, eye, mucous membrane, or parenteral contact with blood and other potentially infectious materials, (i.e. tears, salvia, semen, vaginal secretions, cerebrospinal, synovial, pleural, pericardial, peritoneal, and amniotic fluid) can be reasonably anticipated. Job classifications in which some personnel have occupational exposure to bloodborne pathogens. Records Clerks, Part-Time Records Clerks, Records Supervisors and volunteers who provide fingerprinting services to the public. Tasks and procedures in which occupational exposure to bloodborne pathogens may occur. (These tasks and procedures are performed by personnel in the job classifications listed above). Arrests and Searches (All Types) Motor Vehicle Crash Investigation Delivery of First Aid and CPR Evidence and Property Collection Evidence and Property Handling Processing Prisoners and Fingerprinting Decontamination Procedures General Housekeeping Procedures Transport and Disposal of Bio-Hazardous Waste Physical and Defensive Tactics Training UNIVERSAL PRECAUTIONS 4.1.3 The concept of Universal Precautions (UP) was originally developed by the Center for Disease Control (CDC), as the approach to infection control due to exposure to all human blood and certain human body fluids. The basic concept of the Universal Precautions is that all human blood and certain human body fluids are treated as if known to be infectious with HIV, HBV, and other bloodborne pathogen and diseases. 4.1.4 The Police Department emphasizes the need to treat blood, blood components, saliva, tears, breast milk, semen, vaginal secretions, cerebrospinal fluid, amniotic fluid, urine, feces, and vomitus from all persons, as potentially infectious. 4.1-3 4.1.5 Universal Precautions shall be observed by all personnel to prevent contact with blood or other potentially infectious materials. Failure to comply with the Universal Precautions is a serious department violation and will be handled as such. 4.1.6 Appropriate protective equipment will be used by all personnel unless the member shows that they temporarily and briefly declined to use the personal protective equipment when, under rare and extraordinary circumstances, it was the member’s professional judgment that in the specific instance its use would have prevented the delivery of vital law enforcement/public safety services or would have posed an increased hazard to the safety of the worker or co-workers. PROCEDURES 4.1.7 Disposable gloves shall be worn when handling any persons, clothing or equipment with bodily fluids on them. 4.1.8 Plastic mouthpieces or other authorized barrier/ resuscitation devices shall be used whenever an officer performs CPR or mouth-to-mouth resuscitation. 4.1.9 All sharp instruments such as knives, scalpels and needles shall be handled with extraordinary care, and; shall be considered contaminated items. • Members shall use due care when placing their hands in areas where sharp instruments might be hidden. An initial visual search of the area should be conducted, using a flashlight where necessary. • Needles shall not be recapped, bent, broken, removed from a disposable syringe or otherwise manipulated by hand. • Needles shall be placed in a puncture-resistant container when being collected for evidentiary or disposal purposes. 4.1.10 A disposal receptacle for sharps is available to all members in the agency’s sally port area. 4.1.11 Officers shall not smoke, eat, drink or apply makeup around body fluid spills. 4.1.12 Any evidence contaminated with body fluids will be dried, double bagged in plastic bags and marked to identify potential or known communicable disease contamination. TRANSPORT AND CUSTODY 4.1.13 Members shall avoid putting their fingers in or near person’s mouth. 4.1.14 Individuals with body fluids on their persons shall be transported in separate vehicles from other individuals. 4.1-4 4.1.15 Officers have an obligation to notify relevant support personnel during a transfer of custody when the suspect has body fluids present on his/her person, or has stated that they have a communicable disease. 4.1.16 Suspects taken into custody with body fluids on their persons shall be directly placed in the designated holding area for processing. The holding areas shall be posted with a sign, “Infectious Disease Contamination.” 4.1.17 Officers shall document on the appropriate arrest or incident form when a suspect taken into cus tody has body fluids on his person, or has stated that he has a communicable disease. DISINFECTION 4.1.18 Any unprotected skin surfaces that come into contact with body fluids shall be immediately and thoroughly washed with hot running water and soap for 15 seconds before rinsing and drying. • Alcohol or antiseptic disposable towels may be used where soap and water are unavailable. • Disposable gloves should be rinsed before removal. The hands and forearms should then be washed. • All open cuts and abrasions should be covered with waterproof bandages before reporting for duty. 4.1.19 Officers should remove clothing that has been contaminated with body fluids as soon as practical. Any contacted skin area should then be cleansed in the prescribed fashion. Contaminated clothing should be handled carefully and placed in a biohazard bag for laundering. 4.1.20 The supervisor shall make arrangements to deliver the contaminated clothing to the appropriate Support Services Personnel for transport to the agency’s designated uniform cleaner. The cleaner will be made aware of the biohazerdous contamination. The designated cleaner will wash the clothing in a commercial washer at a temperature of approximately 200 degrees in accordance with requirements for proper cleaning and disinfection. 4.1.21 Under circumstances of extreme contamination the supervisor may approve the disposal of the clothing as opposed to cleaning. If this occurs, the clothing will be properly packaged and placed in a biohazard receptacle. 4.1.22 A supervisor shall be notified and disinfection procedures initiated when ever body fluids are spilled, or an individual with body fluids on his person is transported in a departmental vehicle. 4.1.23 Affected areas shall be immediately designated by the posting of an “Infectious Disease Contamination” sign while awaiting disinfection. 4.1.24 The work environment shall be maintained in a clean and sanitary condition at all times. 4.1.25 Personnel shall remove any excess body fluids from the vehicle with an absorbent cloth, paying special attention to any cracks, crevices or seams that may be holding excess fluid. 4.1-5 4.1.26 The effected area should be disinfected using hot water and detergent and alcohol, and allowed to air dry. 4.1.27 Non-disposable equipment and areas upon which body fluids have been spilled shall be disinfected as follows: • Any excess of body fluids should first be wiped up with approved disposable absorbent materials. • A freshly prepared solution of one part bleach to 10 parts water or a fungicidal/mycrobactericidal disinfectant shall be used to clean the area or equipment. 4.1.28 All disposable equipment, cleaning materials or evidence contaminated with body fluids shall be bagged and disposed of in compliance with state law provisions for disposal of biologically hazardous waste material. A biohazard trash receptacle is available to all members in the agency’s sally port area. 4.1.29 The Evidence Section Supervisor shall be responsible for monitoring all biohazard and sharps receptacles. When the receptacles are getting close to full, the designated biohazard waste pick up vendor will be notified to respond. SUPPLIES 4.1.30 Supervisors are responsible for continuously maintaining and storing in a convenient location an adequate amount of communicable disease control supplies for their unit. 4.1.31 Supervisors are responsible for dissemination of supplies for infectious disease control. Protec tive gloves, other first aid supplies and disinfecting materials will be made readily available at all times. 4.1.32 All departmental vehicles shall be continuously stocked with the following communicable disease control supplies: • Disposable gloves • Puncture-resistant containers and sealable plastic bags • Barrier resuscitation equipment, goggles • Germicidal cleaner • Disposable towels (70 percent isopropyl alcohol) • Waterproof bandages • Absorbent cleaning materials • “Infectious Disease Contamination” signs 4.1-6 4.1.33 Offices using supplies stored in police vehicles are responsible for their immediate replacement. 4.1.34 Officers are required to keep disposable gloves in their possession while in a vehicle or on foot. HEPATITIS B VACCINATION 4.1.35 All employees subject to the Exposure Control Plan (ECP), will be offered immunization against Hepatitis B under the supervision of a licensed physician or a licensed healthcare professional, at no cost. The risks and benefits of immunization will be explained to all employees, and informed consent obtained prior to immunization. 4.1.36 The Hepatitis B vaccine and vaccination series must be offered within 10 working days of initial assignment to employees who have occupational exposure to blood or other potentially infectious materials. 4.1.37 Employees may refuse immunizations subject to the (ECP), or may submit proof of previous immunization. Employees who refuse or accept the immunization will be required to sign a Hepatitis B Refusal/Request Immunization Form (Attachment 4.1-B). Employees who initially refuse immunization may later receive immunization(s) upon request at no cost. POST EXPOSURE EVALUATION AND FOLLOW-UP 4.1.38 Any member who has had unprotected physical contact with body fluids of another person while in the line of duty shall be considered to have been exposed to a communicable disease. (Refer to levels of exposure under Definitions) 4.1.39 A supervisor shall be contacted and a Supervisor’s Accident Investigation Report Form (At tachment 4.1 – A) shall be completed by the supervisor as well as an Exposure Incident Form (Attachment 4.1 – C) for all levels of exposure besides a Casual Exposure. The only reason that a Casual Exposure would be reported is if there was knowledge that the source person was infected with an airborne transmitted disease such as Tuberculoses. 4.1.40 For a Minimal Exposure, thorough disinfections by prescribed procedures shall occur. 4.1.41 For Moderate and Significant Exposures, immediate disinfection procedures should be initiated. The officer shall be transported to the appropriate health care facility for clinical and serological testing for evidence of infection, as soon as possible after the exposure. • The department and Risk Management shall ensure continued testing of the officer for evidence of infection and provide psychological counseling as determined necessary by the health care official. • Members shall receive a copy of the health care provider’s written opinion within 15 days of the evaluation and information on any conditions resulting from the exposure that require further evaluation and treatment. • Unless disclosure to an appropriate departmental official is authorized by the officer or by state law, the officer’s test results shall remain confidential. 4.1-7 4.1.42 Any person responsible for potentially exposing the officer to a communicable disease shall be encouraged to undergo testing to determine if the person has a communicable disease. If the source person refuses, a court order may be obtained. This will be coordinated through Risk Management. • The person and the officer shall be provided a copy of the test results and guaranteed its confidentiality. • Criminal charges may be sought against any person who intentionally acts to expose and officer to a communicable disease. 4.1.43 Officers who test positive for a communicable disease may continue working as long as they maintain acceptable performance and do not pose a safety and health threat to themselves, the public or the department. • The department shall make all decisions concerning the employee’s work status solely on the medical opinions and advice of the department’s health care officials. • The department may require an employee to be examined by department health care officials to determine if he is able to perform his duties without hazard to himself or others. 4.1.44 All personnel shall treat employees who have contracted a communicable disease fairly, cour teously and with dignity. RECORD KEEPING 4.1.45 The department shall maintain written records of all incidents involving employees who have potentially been exposed to a communicable disease while acting in the line of duty. The records shall be stored in a secured area with limited access, and maintained in conformance with applicable privacy laws. 4.1.46 The Exposure Control Plan will be reviewed at least annually for revisions or modifications to accepted protocols. 4.1.47 The training section shall ensure that complete records are maintained on member training to include information on the dates and content of training sessions, names and qualifications of persons conducting the training, and the names and job titles of all persons attending the training sessions. 4.1.48 Training and medical records for each member with occupational exposure shall be maintained in accordance with General Schedule for State Government Agencies (GS1-S). 4.1.49 The DeLand Police Department will maintain records in accordance with OSHA’S CFR 29, Part 1910.1030. Employee participation in the Exposure Control Plan will be documented, including: 4.1-8 Name and SSN of employee Immunization record Circumstances of exposure to communicable disease(s) Post- exposure medical evaluation, treatment, and follow-up Exposure control training 4.1.50 Exposure control records will become a part of the employee’s personal health file and will be maintained for the duration of employment plus thirty ( 30 ) years. 4.1.51 Employee personal health files are strictly confidential. These files will be maintained by the DeLand Police Department. Employee personal health files will not be released without the signed written consent of the employee. 4.1.52 Employees may examine their own personal health files and may request copies be sent to their personal physician. Release of health files will be made only with the signed consent of the employee. TRAINING 4.1.53 The agency shall ensure training to all members with a risk of occupational exposure, a complete course of instruction on the prevention of blood borne diseases prior to their initial assignment. The training shall consist of the following: Familiarization with the agency’s Exposure Control Plan Familiarization with the basic epidemiology, symptoms, and the modes of transmissions of infectious diseases An explanation of the use and limitations of methods that will prevent or reduce exposure, including personal protective equipment. Information about the agency’s hepatitis B vaccination program An explanation of procedures to follow at any incident involving blood or other potentially infectious materials. An explanation of procedures to follow if an exposure occurs, including reporting requirements and medical follow-up An explanation of the signs, labels, and color coding identifying biohazardous waste Familiarization with the agency’s biohazardous waste disposal procedures 4.1-9 Members will have an opportunity to have questions answered related to this training. 4.1.54 All affected members shall receive refresher training and additional training whenever job tasks or procedures are modified in a manner that may alter the risk of exposure or as required by the Chief of Police. ATTACHMENTS 4.1-A Supervisor’s Accident Investigation Report Form. 4.1-B Hepatitis B Refusal/Request Form 4.1-C Exposure Incident Form DRAFTED: PCG-02/2004 REVISED: PCG-04/2004 REVIEWED: GRB- 02/2005 REVISED: GRB-11/2006 REVIEWED: GRB- 03/2007 REVIEWED: JFA—01/2008 REVIEWED: JFA—01/2009 REVIEWED: JFA—02/2010 REVIEWED: JFA – 02/2011 4.1-10