Allergic Reaction/Sensitivity - Food
advertisement

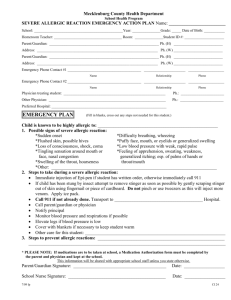
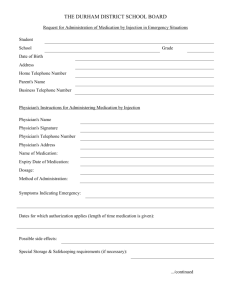
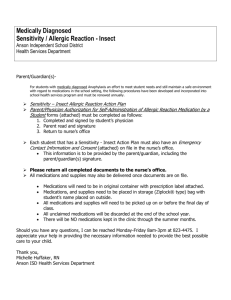
Allergic Reaction/Sensitivity - Latex Anson Independent School District Health Services Department Parent/Guardian(s)In order for the Anson ISD Health Department and/or a student to administer allergic reaction medications at school, Latex Sensitivity – Allergic Reaction Action Plan Parent/Physician Authorization for Self-Administration of Allergic Reaction Medication by a Student forms (attached) must be completed as follows: 1. Completed and signed by student’s physician 2. Parent read and signature 3. Return to nurse’s office Each student that has a Latex Sensitivity Action Plan must also have an Emergency Contact Information and Consent (attached) on file in the nurse’s office. This information is to be provided by the parent/guardian, including the parent/guardian(s) signature. Please return all completed documents to the nurse’s office. All medications and supplies may also be delivered once documents are on file. Medications will need to be in original container with prescription label attached. Medications, and supplies need to be placed in storage (Ziplock® type) bag with student’s name placed on outside. All medications and supplies will need to be picked up on or before the final day of class. All unclaimed medications will be discarded at the end of the school year. There will be NO medications kept in the clinic through the summer months. Should you have any questions, I can be reached Monday-Friday 8am-3pm at 823-4475. I appreciate your help in providing the necessary information needed to provide the best possible care to your child. Thank you, Michelle Huffaker, RN Anson ISD Health Services Department Allergic Reaction/Sensitivity – Latex Emergency Action Plan Anson Independent School District Health Services Department Latex Sensitivity to: Latex: _______________________ Type of Reaction: □ Breathing Difficulty □ Rash □ Hives Has Student been diagnosed with Asthma? □ Yes □ No Medication given at school: ______________ Symptoms Emergency Treatment to be completed by Physician Mild Symptoms (Local reaction) * Mild skin reactions Hives/Swelling only in the areas of allergen contact. Students with an Epi-pen or history of anaphylaxis must go home With parental supervision for the remainder of the school day. SYMPTOMS CAN BECOME MORE SERIOUS VERY QUICKLY OR OVER THE NEXT SEVERAL HOURS. »IF STUDENT HAS MILD SYMPTOMS OR INGESTED IS SUSPECTED: CALL 911 Note time _____________ and stay with student Watch closely for serious symptoms Give _______________________ as ordered by physician Call parent or emergency contact Stay with student until parent or EMS arrives Call school nurse DO NOT HESITATE TO CALL 911 OR TO GIVE EMERGENCY MEDICATION(S) SERIOUS SYMPTOMS (Systemic Reaction): Skin Mouth Throat Gut Lungs Heart widespread hives and flushing, widespread swelling swelling of the tongue itching, or a sense of tightness of the throat, Hoarseness, hacking cough vomiting, nausea, cramps, diarrhea repetitive coughing, wheezing, trouble breathing rapid heart rate, lightheadness, dizziness, loss of consciousness IF STUDENT HAS ANY SERIOUS SYMPTOMS: Note time _____________ and stay with student Give ___________________ as ordered by physician Administer Epi-pen. Follow directions on injection Device as trained. Note time given ______________ Call 911: ask for Advance Life Support for an Allergic reaction Call parent or emergency contacts Call school nurse This Emergency Action Plan must be signed by both parent/guardian and physician My signature below shows I reviewed and agree with this plan. ___________________________________ ______________ Parent Signature Date __________________________________ ____________ Physician Signature Date _______________________________________________ Physician’s Printed Name Allergic Reaction/Sensitivity – Latex Emergency Contact Information and Consent Anson Independent School District Health Services Department Student Name: ____________________________________ Teacher _____________ Student Food Allergies: _________________________________________________ _________________________________________________ _________________________________________________ Student Medication Allergies: ____________________________________________ ____________________________________________ ____________________________________________ Grade: __________ Male: ___ Female: ___ Date of Birth: ___________________ Address: ____________________________ ____________________________ ____________________________ Home Phone: __________________ Cell Phone: ___________________ Emergency No.: ________________ Father’s Name: _____________________________ Work Phone: ______________ Cell Phone _______________ Mother’s Name: ____________________________ Work Phone: _______________ Cell Phone _______________ In case parents can not be reached at time of emergency, please call: Name: _________________________________ Phone: _______________________ Relationship to student: _________________ Phone: ________________________ Name: _________________________________ Phone: _______________________ Relationship to student: _________________ Phone: ________________________ Unfortunately, there is always the possibility of an accident occurring to a student at school or while participating in an after-school activity. In case an accident should occur, the school and/or the UIL does not assume responsibility. Nevertheless, if an accident should occur, a discretionary judgment will be made by a school representative in regard to the student’s need for immediate care and treatment. Therefore, I do herby request, authorize, and consent to such care and treatment as may be given to the said student by and physician, trainer, nurse or school representative. As well, I do hereby agree to indemnify and save harmless the school and any school representative from any claim by any person whomsoever on account of such care and treatment of the said student. Between this date and the end of the school year, illness or injury could occur that may limit the student’s participation, I agree to notify the school authorities of such illness or injury. ________________________________ Signature of Parent/Guardian _________________________ Date ______________________________ _______________________ Signature of Parent/Guardian Date Allergic Reaction/Sensitivity – Latex Parent/Physician Authorization for Self-Administration of Allergy Medication By a Student Anson Independent School District Health Services Department Parent Authorization I have reviewed the attached guidelines and procedures for Self-Administration of Prescription Anaphylaxis Medication by Students; discussed them with my child; and request that my child be able to possess and selfadminister his/her prescription anaphylaxis medication while on school property or at a school-related event or activity. I understand that the anaphylaxis medication must be prescribed for my child as indicated on the prescription label, which must be affixed to the medication container (inhaler canister or packaging box). I release the school district and employees of any liability arising from self-administration. _____________________________________________________ Parent/Guardian Signature ___________________________ Date Physician Authorization The medical history and my examination of _______________________________________________, Students Name indicates that he/she does have anaphylaxis. The student has been educated and is knowledgeable about his/her anaphylaxis and can properly self-administer the prescribed medication and determine its effectiveness. Name of Medication: __________________________________________________________________ Purpose of Medication: _________________________________________________________________ Prescribed Dosage: ____________________________________________________________________ Times at which or circumstances under which the medicine may be administered: _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ Period of time for which the medicine has been prescribed: □ Long Term (chronic condition) □ Short Term and should be discontinued by ________________________ Date ________________________________________ Physician’s Printed Name ________________________________________ Physician’s Signature Office Telephone Number: ______________________________________ Diagnosed Medical Condition Latex Sensitivity – Allergic Reaction - Anaphylaxis Waiver of Treatment Anson Independent School District My child, _________________________________ has been medically diagnosed and/or treated for Latex Sensitivity – Allergic Reaction and I have been informed by Anson ISD, school personnel of the required documentation needed to properly treat him / her while at school and/or school related events. I understand that it is my responsibility to provide to the school all needed information and medication. However, I decline to participate in the requirements. Therefore, I do herby agree to indemnify and save harmless the Anson ISD and any of its representatives from any liability arising in the event that my child, listed above, have an Latex Sensitivity and/or Allergy-like related episode. ________________________________________ Parent Signature __________________________ Date ________________________________________ Parent Printed Name ___________________________ Phone Number