Lab 8

BIOLOGY 1001
WEEK 9 LABORATORY
FALL 2004
Genetics and Inheritance
Genetics is the study of inheritance. We can trace its scientific beginnings to the work of Gregor
Mendel. He was the first to show that traits are controlled by what we now call genes and that there are alternative forms to each gene, called alleles.
In the pea plants he worked on, as in all diploid organisms, there are two copies, two alleles, of each gene and they may be the same or different. When cells divide mitotically, each daughter cell receives one of each allele so its genetic makeup is identical to the parent cell. When cells divide meiotically, producing haploid cells, only one of the two alleles goes into each daughter cell. The two alleles become separated or segregated from each other. Of the four daughter cells in meiosis, two get copies of one allele, the other two cells get copies of the other allele. This is the essence Mendel's first law.
When we follow the inheritance of two genes, two pairs of alleles, then Mendel's second law says that the segregation of the first pair will be independent of the segregation of the second pair. We know there are many exceptions to Mendel's two laws. For example, genes can be on the same chromosome so that they do not segregate independently but stay together or "linked.” The seven traits Mendel worked with happened to be determined by genes on pea’s seven different chromosomes. There has been speculation about whether Mendel “cheated” in only choosing to study the traits whose results supported his hypotheses.
Individuals can have more than two sets of chromosomes and therefore more than two alleles for any one gene. For example, some plants are polyploid with more than two complete sets of chromosomes, as in triploids (3n) or tetraploids (4n). Some plants and animals are aneuploid and have one or two additional (or fewer) chromosomes than the typical diploid number, as in trisomics (2n + 1) or monosomics (2n - 1). However, these exceptions do not tarnish Mendel's reputation or deny the utility of his laws. Please note that Mendel’s laws cannot be applied easily to polyploid or aneuploid organisms.
One consequence of Mendel's law is that they enable us to have such a high level of confidence in the results from previous experiments on inheritance that we are able to predict the outcome of future experiments of the same type. Thus, observed results should not differ significantly from expected results. A statistical test called the Chi Square test is often used to determine whether there are significant differences between observed and expected results.
In laboratory today, you will observe the behavior of single allelic pairs that determine corn kernal color and learn how to perform Chi Square tests. You will investigate multiple alleles (more than two in a population) by determining ABO blood types and examine the genetics of other human traits, such as tongue rolling.
I. Monohybrid cross and the Chi square test: Corn kernel color
II. Multiple alleles: Human blood types (ABO and Rh)
III. Individual genetic make-up
Textbook reading prior to coming to lab: Tobin and Dusheck, 2 nd edition: pp. 164-191.
Lab 9-1
I. MONOHYBRID CROSS AND THE CHI SQUARE TEST: CORN KERNEL COLOR
In this week's lab we will conduct a small survey on the inheritance of color in corn. Purple pigment is the dominant color in corn and is represented by R . The R allele encodes a functional copy of an enzyme involved in purple pigment biosynthesis; the r allele does not encode a functional copy of the enzyme. Yellow pigment is the recessive color and is represented by r .
The possible genotypes and phenotypes with respect to color are:
Genotype Phenotype
RR (homozygous dominant)
Rr (heterozygous)
Purple
Purple
(in this case, just one copy of the functional enzyme is enough to make the purple pigment) rr (homozygous recessive)
The genetic history of your corn is:
Parental Generation (P)
Yellow
RR x rr
(purple) x (yellow) resulting in:
First Filial Generation (F
1
) Rr
(heterozygous purple)
If we cross two members of the First Filial Generation, F
1
,
Rr x Rr in the Second Filial Generation (F
2
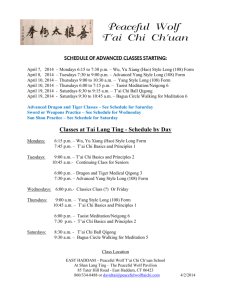
), we will obtain a phenotypic ratio of 3 purple:1 yellow and a genotypic ratio of 1 homozygous purple: 2 heterozygous purple: 1 homozygous yellow.
Lab 8-2
Parental Generation (P)
First Filial Generation (F
1
)
RR genotype rr genotype
(purple phenotype) (yellow phenotype)
Punnett square
Second Filial Generation (F
2
)
2
1
1
R r
R
RR
Rr r
Rr rr
genotype phenotype
RR (homozygous) purple
Rr (heterozygous) purple rr (homozygous) yellow genotype ratio: 1RR: 2Rr: 1rr
R
R r
Rr
Rr r
Rr
Rr
Rr (heterozygous) genotype, purple phenotype phenotype ratio: 3 purple: 1 yellow
Lab 8-3
Working with another student in lab, count 100 kernels of the F
2
generation from a cross of two heterozygous purple plants. What phenotypic ratio would you expect in the offspring from such a cross?
Compute the Chi Square value for your data as shown below. Your instructor will total the class data and calculate a Chi Square test for your lab section's data. Record the results in Table 8-1.
CALCULATIONS
Suppose that today, after counting the corn seeds, we observe a ratio of 70 purple to 30 yellow.
Is this ratio close to the 3:1 ratio that we predicted? Can we safely assume that the deviation was due to chance alone? How close must observed and predicted ratios be to conclude that our results meet expectations?
The Chi Square test is a useful statistical test to evaluate the difference between observed and expected results. We use the Chi Square test to compare observed and expected data given a particular model, e.g., a 3:1 ratio. A significant outcome tells us that there is a difference between actual and predicted results that is not due to chance. In such a case, you would need to reconsider your model.
The formula for Chi Square (
2
) is
2 =
(O-E) 2
E
And may be calculated as follows:
EXPERIMENT #1
1 st
phenotype
(purple)
2 nd
phenotype
(yellow)
Observed value (O)
Expected value (E)
70
75
30
25
(O-E)
(O-E)
(O-E)
2
2
/E
-5
25
25/75 = 0.3
+5
25
25/25 = 1.0
Chi Square
2
=
(O-E)
2
/E 1.3
Lab 8-4
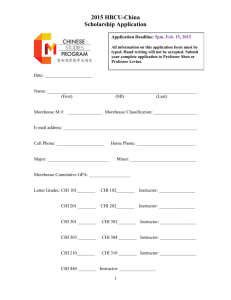
To interpret our Chi Square value of 1.3 we must refer to Table 8-2. The table gives different
Chi Square values for several degrees of freedom , with the probability associated with each Chi
Square value across the top. The number of degrees of freedom for the Chi Square test is always one less than the total number of classes. In our case, we are dealing with two classes: 1) purple corn and 2) yellow corn. Therefore, 2 classes - 1 class = 1 degree of freedom.
Probability ( P-value ) refers to the percent of time when differences between observed and expected data are due to chance. The P-value is expressed in values between 0 and 1. One means that 100% of the time the deviation of the observed values from the expected values is due to chance, while 0.20 means that 20% of the time the deviation of the observed values from the expected values is due to chance.
Statisticians have decided that a probability greater than 0.05 is not significant. Simply put:
If P > 0.05 the deviation is not significant and is due to chance ; this means that there is a greater than 5% probability that the deviation of the observed values from the expected values is due to chance.
If P = or < 0.05 the deviation is significant and is not due to chance; this means that there is a less than 5% probability that the deviation of the observed values from the expected values is due to chance.
We must now compare our Chi Square value to the Chi Square values listed for one degree of freedom. The greater the Chi Square value, or the more to the right side of the table, the more statistically significant will be the deviation between observed and expected.
Our Chi Square value of 1.3 agrees most closely with the value of 1.64 shown in the left-most column of probabilities. Since this deviation yields a probability greater than 0.20, it cannot be regarded as statistically significant. We may conclude that there is a probability greater than 20% that the deviation is due to chance. Our observed results agree well enough with our predicted results and we need not modify the assumptions upon which we based our predictions.
Lab 8-5
Now let us calculate the Chi Square value for an experiment where the observed values are 50% purple and 50% yellow:
EXPERIMENT #2
Observed value (O)
1 st
phenotype
(purple)
2 nd
phenotype
(yellow)
Expected value (E)
50
75
50
25
(O-E)
(O-E)
2
-25
625
+25
625
(O-E)
2
/E
625/75=8.33
33.3
625/25=25
Chi Square
2
=
(O-E)
2
/E
Referring back to the table and one degree of freedom, a Chi Square value equal to or greater than 10.83 has a chance or probability of 0.001, or 1 in a 1000. Our Chi Square value of 33.3 is greater than 10.83. Therefore, a deviation due to chance alone in this experiment occurs less than
0.1% of the time.
Recall that statisticians have decided that a ( P ) equal to or less than 0.05 (5%) is considered significant. Since the deviation in our second experiment has a chance or probability of less than
0.001, it is regarded as statistically significant. We may conclude that the deviation in this second experiment is not due to chance and therefore cannot be disregarded.
We are forced to reevaluate our experiment's hypothesis and methods so that we may establish whether our initial expectations need revising.
One should not confuse the Chi Square and the t-test. The criteria for significance do not differ between the tests. What does differ is the question that is being asked in each case. When performing the t-test an experimenter asks: Do two groups differ from each other with respect to a certain variable? A significant difference gives an affirmative response to this question: Yes, the two groups do differ.
When performing the Chi Square test, however, we ask a different question: Do our observed results match our expected results? A significant difference gives a negative response to this question: No, the results do not match our expectations. If our observed results do not match expected results, the hypothesis we used to determine expected results will probably need to be revised.
Lab 8-6
TABLE 8-1 . DATA SHEET FOR KERNEL COLOR
INDIVIDUAL DATA
Observed value (O)
1 st
phenotype
(purple)
Expected value (E)
(O-E)
(O-E)
2
(O-E)
2
/E
Chi Square
2
=
(O-E)
2
/E
CLASS DATA
Observed value (O)
1 st
phenotype
(purple)
Expected value (E)
(O-E)
(O-E)
(O-E)
2
2 /E
Chi Square
2
=
(O-E)
2
/E
2 nd
phenotype
(yellow)
2 nd
phenotype
(yellow)
Lab 8-7
TABLE 8-2 . INTERPRETING CHI SQUARE VALUES
To interpret a Chi Square value, we must determine the degrees of freedom and refer to the Chi
Square table. The number of degrees of freedom (df) for the Chi Square test is always one less than the total number of classes (df = N - 1).
The table below shows seven different Chi Square values for each of a series of different degrees of freedom, and gives the probability ( p ) that deviation as great as or greater than that represented by each Chi-square value would occur strictly by chance.
The critical value, where p = 0.05, is taken by statisticians as the point which determines whether the deviation in an experiment is significant or not. p = 0.05 means that the incidence of a deviation occurring by chance will be one out of 20 or 5% of the time.
For example, a Chi Square value for 1 degree of freedom at p = 0.05 is 3.84. This number is the critical value for that degree of freedom. Any Chi Square value equal to or greater than 3.84 would therefore be statistically significant.
Note that statistical significance does not necessarily tell us about biological significance. A difference can be statistically significant without being biologically significant. Likewise, a difference can be biologically significant without being statistically significant. The use of statistics can help us scientists analyze data, but be cautious about the conclusions you draw.
When p > 0.05 the deviation is not significant and is due to chance.
When p < 0.05 the deviation is significant and is not due to chance.
Chi-Square Distribution
Degrees of
Freedom .90
1
2
3
4
.02
.21
.58
1.06
1.61 5
6
7
8
9
10
2.20
2.83
3.49
4.17
4.86
.70
.15
.71
1.42
2.20
3.00
3.83
4.67
5.53
6.39
7.27
.50
.46
1.39
2.37
3.36
4.35
5.35
6.35
7.34
8.34
9.34
Probability
.30
1.07
2.41
3.66
4.88
6.06
7.23
8.38
9.52
10.66
11.78
.10
2.71
No statistically significant difference between observed and expected values
(variation is due to chance)
4.60
6.25
7.78
9.24
10.64
12.02
13.36
14.68
15.99
.05
3.84
5.99
7.82
9.49
11.07
12.59
14.07
15.51
16.92
18.31
.01
6.64
9.21
11.34
13.28
15.09
16.81
18.48
20.09
21.67
23.21
Statistically significant difference
(variation is not due to chance)
Lab 8-8
II. MULTIPLE ALLELES: HUMAN BLOOD TYPES (ABO and Rh)
An example of inheritance where more than simple dominance and recessiveness occurs is in the inheritance of the ABO blood groups. In this type of inheritance, genes exist in more than two allelic forms, so there are more phenotypic possibilities.
The ABO classification is based upon the characteristics of specific protein molecules ( antigens ) located on the surface of red blood cells. The molecular structure of each antigen is unique and dictated by specific genes.
Humans have an immune system that recognizes and protects all that is "self" from all that is foreign and "non-self". Antibodies , specific proteins made by the immune system, inactivate foreign blood antigens.
The following chart illustrates the antigen, protein, and antibody components of the four blood types possible under the ABO classification system. Note that each blood type will make antibodies against whatever antigen is not present in its own type, with type O making antibodies against both A and B antigens. If an individual were to be accidentally transfused with the wrong type of blood, clumping or agglutination of red blood cells would occur.
Phenotype Genotype Cellular Antigen Plasma Antibodies
O ii none anti-A and anti-B
A
B
I
A
I
A
or I
A i
I B I B or I B i
A
B anti-B anti-A
AB I
A
I
B
A and B none
The Rh classification scheme (Rh+/Rh-) is also based on the presence of antigens on red blood cells. More information on the Rh factor is included on the next page.
To determine someone’s blood type, three reagents are needed: one containing anti-A antibodies, one containing anti-B antibodies, and one containing anti-Rh antibodies. Each of the antibody solutions should cause the red blood cells containing the corresponding antigen to clot.
We will be testing a sterile, non-pathogenic, blood-like substance in lab this week. Although almost all of us think it would be great if you could determine your own blood type, health concerns prevent us from being able to conduct such an experiment in this lab. The risk of exposure to infectious agents is simply too real to overlook. While we’re on the subject, many serious infectious agents can be transferred through bodily fluids such as blood. The most life-threatening risks would be HIV and hepatitis. Please minimize your risk of infection by not sharing bodily fluids with others. If you do not engage in risky behavior, you might consider donating your blood. There is a large demand for blood products, no matter what your blood type, and you can help those who are in medical need. Donated blood is collected carefully by trained technicians who use sterile materials so that there is no risk of infection to the blood donor. Blood is then screened for multiple infectious agents before it can be used in transfusions.
Lab 8-9
Rh Blood Types from http://anthro.palomar.edu/blood/Rh_system.htm
“Rh blood types were discovered in 1940 by Karl Landsteiner and Alexander Wiener. This was 40 years after Landsteiner had discovered the ABO blood groups. Over the last quarter century, we have learned far more about the processes responsible for
Rh types.
This blood group may be the most complex genetically of all blood type systems since it involves 45 different antigens on the surface of red cells that are controlled by 2 closely linked genes on chromosome 1.
The Rh system was named after rhesus monkeys, since they were initially involved in the research to make the antiserum
[containing the antibodies] for typing blood samples. If the antiserum agglutinates your red cells, you are Rh+ and if it doesn't, you are Rh- . Despite its actual genetic complexity, the inheritance of this trait usually can be predicted by a simple conceptual model in which there are two alleles, D and d. Individuals who are homozygous dominant (DD) or heterozygous (Dd) are Rh+.
Those who are homozygous recessive (dd) are Rh- (i.e., they do not have the key Rh antigens).
Clinically, the Rh factor, like ABO factors, can lead to serious medical complications. The greatest problem with the Rh group is not so much incompatibilities following transfusions (though they can occur) as those between a mother and her developing fetus.
Mother-fetus incompatibilities occur when the mother is Rh- (dd) and the father is Rh+ (DD or Dd). Maternal antibodies can cross the placenta and destroy fetal red blood cells. The risk increases with each pregnancy.
Rh type mother-fetus incompatibilities occur only when an Rh+ father successfully mates with an Rh- mother. The first time an
Rh- woman is pregnant, there usually is not incompatibility difficulty for her Rh+ fetus. However, the second and subsequent births are likely to have serious problems. In order to understand why first born are normally safe and later children are not, it is necessary to understand some of the placenta's function. Nutrients and the mother's antibodies regularly transfer across the placental boundary into the fetus, but her red blood cells usually do not (except in the case of an accidental rupture). Normally, anti-Rh+ antibodies do not exist in the first-time mother unless she has previously come in contact with Rh+ blood. Therefore, her antibodies are not likely to agglutinate the red blood cells of her Rh+ fetus.
Placental ruptures do occur normally at birth so that some fetal blood gets into the mother's system, stimulating the development of antibodies to Rh+ blood antigens. As little as one drop of fetal blood stimulates the production of large amounts of antibodies.
When the next pregnancy occurs, a transfer of antibodies from the mother's system once again takes place across the placental boundary into the fetus. The anti-Rh+ antibodies that she now produces react with the fetal blood, causing most of its red cells to agglutinate. As a result, the newborn baby has severe life-threatening anemia because of a lack of oxygen in the blood. They also are usually jaundiced, fevered, quite swollen, and have an enlarged liver and spleen. This condition is called erythroblastosis fetalis . The standard treatment is immediate massive blood transfusions of Rh+ blood into the baby. This is usually done immediately following birth, but it can be done to the fetus prior to birth.
Erythroblastosis fetalis can be prevented for women at high risk (i.e., Rh- women with Rh+ mates) by administering a serum
(Rho-GAM ) containing anti-Rh+ antibodies around the 28th week of pregnancy and within 72 hours after the delivery of an Rh+ baby. This must be done for the first and all subsequent pregnancies. The injected antibodies quickly agglutinate any fetal red cells as they enter the mother's blood, thereby preventing her from forming her own antibodies. Since the serum given the mother is a passive form of immunization, it will shortly leave her blood stream. Therefore, she does not produce any long-lasting antibodies. This treatment can be 99% effective in preventing erythroblastosis fetalis. Rho-GAM is also routinely given to Rh- women after a miscarriage, an ectopic pregnancy, or an induced abortion.
Anti-Rh+ antibodies may be produced in an individual with Rh- blood as a result of receiving a mismatched blood transfusion.
When this occurs, there is likely to be production of the antibodies throughout life. Once again, Rho-GAM can prevent this from happening.
Mother-fetus incompatibilities can result with the ABO system also. However, they are very rare--less than .1% of births are affected and usually the symptoms are not as severe. It most commonly occurs when the mother is type O and her fetus is A, B, or AB. The symptoms in newborn babies are usually jaundice, mild anemia, and elevated bilirubin levels. These problems are usually treated successfully without blood transfusions.”
Lab 8-10
Blood typing procedure:
1.
Obtain a Blood Test Card.
2.
a.
Place two drops of Anti-A serum (blue) in the circle labeled "Anti-A" and replace the cap. (Always replace the cap on one vial before opening the next vial to prevent cross contamination). b.
Place two drops of Anti-B serum (yellow) in the circle labeled "Anti-B" and replace the cap. c.
Place two drops of Anti-D serum (clear) in the circle labeled “Anti-D” and replace the cap.
1.
Obtain one of the aseptic red blood cell suspensions.
2.
Place two drops of an unknown blood sample (A, B, or C) onto each of the circles labeled
“Blood” on the test card.
3.
Use a blue stirring stick to mix the blood with the Anti-A serum. Carefully spread the blood and serum mixture with the stirring stick until both connecting circles are covered by the mixture. Then discard the stirring stick.
4.
Repeat this procedure with a yellow stirring stick and the Anti-B serum. Be careful not to cross-contaminate your samples because the slightest contamination will make your results inaccurate.
5.
For Rh typing, use a white stirring stick to mix the blood with the Anti-D serum.
6.
Place the slide under a lamp for a few minutes to obtain the Rh results.
7.
If clotting occurs in the Anti-A serum, then the suspension was type A blood. If clotting appears in the Anti-B serum, then the suspension was type B blood. This is because the serum tests for the presence of the antigen or protein, not for the presence of antibodies. If no clotting appears, the suspension was type O blood. If both clot, the suspension was type AB blood. Positive Rh reactions take longer than positive A or B reactions and exhibit finer clotting. In some cases, several minutes will be required to obtain an accurate Rh reading.
11. Which blood sample did you type: ________________ What is the blood type of the suspension according to this test?_________
NOTE: All blood-contaminated implements and cards should be disposed of in the special waste bag provided in your lab room.
Lab 8-11
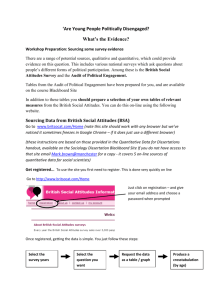
ABO and Rh Blood Type
Frequencies in the United States
ABO Type Rh Type How Many Have It
B
B
AB
AB
O
O
A
A positive 38% negative 7% positive negative positive negative positive negative
34%
6%
9%
2%
3%
1%
45%
40%
11%
4%
(Source: American Association of Blood Banks)
III. INDIVIDUAL GENETIC MAKE-UP
In this part of the exercise you will examine your own phenotype and genotype for several traits, each of which (except for eye color and the Rh factor) is thought to be controlled by a single gene. The pattern of inheritance is given in Table 8-3. Fill in as much as you can.
Lab 8-12
TABLE 8-3. INDIVIDUAL GENETIC MAKE-UP
Trait Inheritance Pattern* Your Phenotype Your Genotype**
ABO blood type
Rh factor
A and B codominant,
O recessive
Autosomal,
Positive dominant
Mid-digital hair
PTC paper tasting
Autosomal,
Dominant
Autosomal,
Dominant
Tongue rolling
Widow’s peak
Hitch-hiker’s thumb
Autosomal,
Dominant
Autosomal,
Dominant
Unattached ear lobes
Autosomal,
Recessive
Autosomal,
(possibly polygenic)
Dominant
Ability to smell
“aparagus urine”
Eye color
Autosomal,
Dominance?
Autosomal, polygenic
Non-blue dominant over blue
Color blindness
X-linked
Recessive
*
Except for “ability to smell…”, information comes from: McKusick, V.A. 1975.
Mendelian
Inheritance in Man. Catalog of Autosomal Dominant, Autosomal Recessive, and X-linked
Phenotypes. Fourth edition. The Johns Hopkins University Press, Baltimore.
** Except for ABO blood type, use upper case for dominance and lower case for recessive for all traits. Example, use W for dominant Widow’s peak and w for recessive no Widow’s peak. If there is more than one possible genotype, please list them all. Simplify the Rh factor to dominant and recessive.
Lab 8-13
I.
BIOLOGY 1001 NAME_____________________________
DATA SHEETS: LABORATORY 8--Genetics and Inheritance
Monohybrid Cross and the Chi Square Test: Corn Kernel Color
Attach the completed data sheet on kernel color (Table 8-1).
Write a brief two paragraphs or so contrasting the t-test and the Chi Square test.
Lab 8-14
II. Multiple Alleles: Human Blood Types (ABO and Rh factor)
What does the term “multiple alleles” mean?
How many allelic forms do the blood types have and what are they? Hint: Look at the genotypes of the different blood types.
II. Individual Genetic Make-up
Attach Table 8-3 on human traits.
Speculate as to why there are not more traits listed.
Lab 8-15