Travel Vaccinations - Green Street Clinic
advertisement

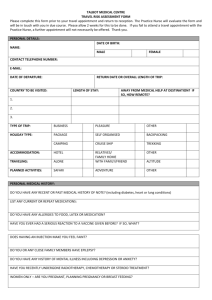
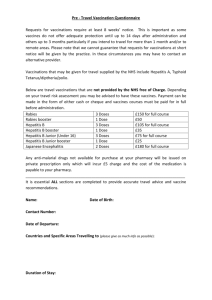
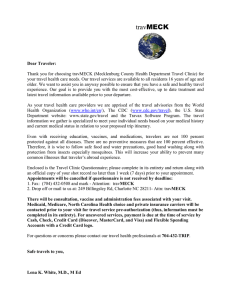
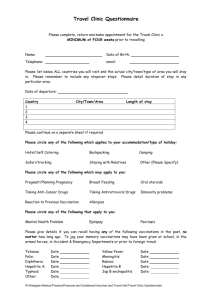
Travel Vaccinations Please complete the attached questionnaire as fully and completely as possible and return to Reception Allow 1 week for the practice nurse to review your record and then contact the surgery to find out which vaccinations you require Please be aware that most vaccines need to be in your system at least two to three weeks before you travel to give the best protection against possible risk of infection A course of vaccines may be required for some destinations, please allow plenty of time before you travel to complete your course A charge is made for some travel vaccines (please see below) Please be aware that most travel vaccinations are not included within NHS services and are offered on a private basis. If we are unable to vaccinate within your timeframe you may have to be seen elsewhere where charges may be considerably higher Japanese Encephalitis Rabies Hepatitis B Meningitis ACWY Tick Encephalitis MMR £178 course of 2 £150 course of 3 £75 course of 3 £40 course of 1 £50 per vaccine £20 course of 1 A private prescription will be provided for malarial treatment Payment for vaccination courses is required prior to your first appointment as some vaccinations have to be ordered in. You need to pay in advance because sometimes patients change their mind and when this happens the practice incurs a cost for the vaccines and may not be able to use them for other patients if the shelf life is too short Cheques should be made payable to Green Street Clinic. Please remember it is the patients’ responsibility to contact the surgery to make an appointment with the practice nurse after completion of the Holiday Vaccination form. Whilst we will always try to accommodate patients who have booked holidays at short notice, at busy times this may not be possible. PLEASE NOTE THAT WE ARE NOT A YELLOW FEVER CLINIC SO IF THIS VACCINE IS NEEDED, YOU WILL NEED TO GO ELSEWHERE. PLEASE ASK PRACTICE NURSE FOR AN UP TO DATE LIST OF CLINICS Please find below alternative sources for travel vaccinations: MASTA Travel Clinic 01273 606636 Apollo Medical Centre 01323 434100 Wish House Clinic 01273 430022 GREEN STREET CLINIC IMMUNISATION FOR FOREIGN TRAVEL Fill in one form for EACH traveller SURNAME _________________________ FIRST NAMES ____________________________ ADDRESS __________________________ TEL NO __________________________ __________________________ ____________________________ AGE __________________________ Which country are you visiting including TOWNS CITIES AND AREAS VISITED ____________________________________________________________________________ When do you leave? __________________________________________ How long are you staying there? _________________________________________ Are you stopping anywhere on the journey? e.g. to change flights YES/NO If YES, where? ________________________________________ and for how long? _________________________ hours/days/weeks Are you staying in a hotel or private home? YES/NO Will you camp or sleep rough? YES/NO Have you been immunised previously against? : TETANUS YES/NO When? _____________ (year) POLIO YES/NO When? _____________ (year) TYPHOID YES/NO When? _____________ (year) MENINGITIS YES/NO When? _____________ (year) CHOLERA YES/NO When? _____________ (year) YELLOW FEVER YES/NO When? _____________ (year) RABIES YES/NO When? _____________ (year) HEPATITIS B YES/NO When? _____________ (year) HEPATITIS A YES/NO When? _____________ (year) Others e.g. RUBELLA YES/NO When? _____________ (year) Do you have any medical problems requiring regular supervision? If YES, what is the problem? YES/NO _________________________________ Are you taking steroids? YES/NO Are you taking any other regular medicines? YES/NO Are you pregnant? YES/NO Have you reacted badly to any previous vaccine? YES/NO If YES, which vaccine? Are you allergic to any medicines? If YES, which? _________________________________ YES/NO _________________________________ I confirm the above answers to be correct to the best of my knowledge and request immunisation as appropriate to my trip together with advice on anti-malarial drugs. PATIENTS SIGNATURE _____________________ DATE ______________________ (parent if under 16)