This manuscript presents the results of a
advertisement

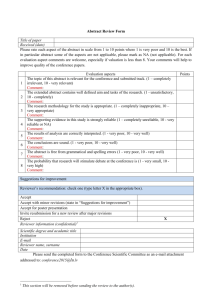
October 1st, 2007 Editor, BMC-series Journals BioMed Central Middlesex House 34-42 Cleveland Street London W1T 4LB Re.: Responses to comments made by reviewer #2 to manuscript submission # MS: 2073626391423293 Dear Sir or Madam, We recently received a rejection letter from BMC Infectious Diseases on a manuscript submitted to you as # MS: 2073626391423293 While the comments of reviewer #1 were appropriate and could easily be addressed in revisions, the manuscript was rejected based on the decision of reviewer #2. Upon reading the comments made by reviewer #2, I began to question whether they had the expertise to make such a decision. I found several instances where information was claimed to be missing that was indeed present in the manuscript. Comments made suggested that they were unfamiliar with the type of study population (anti retroviral treated HIV infected patients) and methods (immunological methods) used in the manuscript. Overall the review was confusing and the nature of their specific objections unclear beyond what would be related to not understanding the field. Since reviewer # 1 appeared to be comfortable with the study design, study population and methods used, I conclude that the problem is not solely in how the manuscript is written. At this juncture I feel strongly that a decision to reject this manuscript based on review #2 is unjustified. I therefore request that the decision to reject be reconsidered. To support this request I have addressed point by point the comments made by reviewer #2 below. Comment 1 General: The authors are assuming that the readers are very well familiar with their terminology and notation when reporting the results of their study as well as familiar with the methods implemented by the authors and the population of study. Response 1: The authors contend that the terminology, methods and study population are standard for the field and should be understandable to an audience that follows the literature on the subject matter. Comment 2: Abstract: -What is PBMCs in the abstract, it is not previously referenced. -what is pre-T1 definition by the authors in this abstract? -What is IQR and r in this abstract? -What is the author’s definition of “drug holiday”? Response 2: These can be defined in a revised manuscript. Comment 3: Background: Please provide the reference for the SMART trial. Response 3: This is already provided in the manuscript as reference #5. Comment 4: Methods: Authors used statistical methods for the description and interpretation of their findings. Authors used statistical inference techniques to report their findings. The use of statistical methods in inferential process is based on the assumption that there is a sample selected from a population of interest. Statistical methods are also known for samples that were randomly selected from the population of interest with some known probability to proceed with the inferential process. The authors lacked to describe the population of interest and how those 13 patients were selected for their analysis. From which country are these patients? Why these patients represent a particular population? Among how many these patients are only available? What was the inclusion and exclusion criteria for these individuals? Why was a retrospective study chosen and from where was that retrospective information collected? Which format, form, or questionnaire was used to collect systematical information on these patients? Why there is not description of the precious drugs used by these patients and why was not important for the authors? It is unclear how other readers will be able to compare their patients with the description of the patients provided here, i.e. other countries? Other hospitals? Response 5: 1) The patients are Canadian and followed at the Immune Deficiency Treatment Centre of the McGill University Health Centre in Montreal, Quebec, Canada. 2) The 13 patients studied are all the individuals found at this site who met the inclusion criteria described in the Materials and Methods section and for whom frozen cell samples were available on which to perform immunological testing. 3) The inclusion criteria are provided in the Materials and Methods section. 4) A retrospective study was chosen because the material existed and the expertise was in place to address the following question: Do pre-treatment interruption parameters determine the extent of viral load rebound and CD4 T cell decline observed in a group of subjects who were unable to control their viral load before they stopped a therapy regimen, and who stopped therapy for long enough to experience a viral rebound. These clinical parameters (viral load and CD4 count change) are surrogate markers of outcome after treatment interruption. 5) The patients were selected using a database that is maintained in our centre of clinical testing results collected at each clinic visit. 6) As this was a retrospective study on an HIV clinic based population the patients had been on multiple treatment regimens. This is typical and representative of a therapy experienced HIV infected population in the real world. The critical issue is that they were all experienced with regard to antiretroviral therapy, had been on many regimens and were experiencing drug failure as defined by detectable viral loads before they stopped therapy. Listing the regimens could be done but would differ from patients to patient and would confuse rather than clarify. 7) These patients should be representative of many HIV infected individuals seen by treating physicians. These are individuals who have been treated for years with multiple regimens, are failing treatment and for one reason or another wish to stop taking antiretroviral therapy for a while. This is a situation encountered by physicians treating HIV infected individuals. Some patients who stop therapy will exhibit a severe decline in CD4 counts and if an educated guess could be made that this will occur could be discouraged from stopping therapy. Other patients will remain stable and in their case stopping therapy will have less negative impact of their disease progression. The manuscript addresses whether certain tests can aid in making this decision. Comment 6: -What was the purpose of dichotomizes the count of CD4+T cell decline? Response 6; The purpose is to view the results in another manner by separating the subjects into the half that did worse versus better based on median value of the outcome measures (CD4 count change) after therapy and compare the value of markers (%CD4+CD57+ cells and proliferative capacity to Gag p55 or cytomegalovirus) before therapy interruption in these 2 groups. Comment 7: -Which subpopulations were studies? It is unclear in this current version of the manuscript. Response 7: The study population remains constant throughout, i.e. the same 13 individuals. Comment 8: -What are the responses evaluated in the figures presented in this paper? They are described differently than in the text or they are different variables presented? Response 8: The response evaluated in figure 1A are flow cytometry plots of CFSE assay showing proliferation to the stimuli/controls listed to the left by cells in the CD4 and CD8 compartments for a representative individual who exhibited a good versus poor outcome following treatment interruption. Figure 1b compiles data for CMV-specific and HIVGag p55-specific proliferation for all individuals tested for CD4+ T cells in the left panels and CD8+ T cells in the right panels. Figure 2 shows representative flow cytometry plots of CD4+CD57+ cells for a patient with low baseline percent CD4+CD57+ T-cells and low CD4 decline during TI (Patient #2) and a patient with high baseline percent CD4+CD57+ T-cells and high CD4 decline during TI (Patient #1). Figure 2b compiles the % CD4+CD57+ values for all study participants versus CD4 changes from baseline to the treatment interruption time point. This information is in the manuscript and legends. It is also a standard way to show results where an example of the research results for an individual are shown in one panel to give a flavor for the quality of the results generated; the results for the study population is then presented in an additional panel with the statistical analysis. Comment 9: -What are the values reported in each contour plot for figures 1, A? -What was the purpose of the individual contour plots? Why was not described in the methods of this manuscript? Response 9: The value in the contour plots for Figure 1A are the %CFSElow positive cells; for figure 2A the percent of CD4+CD57+ cells. As cells labeled with CFSE proliferate and divide the CFSE fluorescent marker intensity is halved with each cell division and therefore becomes dimmer and is detected in a lower fluorescence intensity channel. If this was not made explicit in the text it is because it is a standard technique used in the field. Comment 10: -Why only 13 patients? Response 10: See above Comment 11: -What was the timeframe for collecting these patients? What are the biases associated with this? Response 11: The timeframe for collecting the samples is 5/20/1997 to 7/31/2001. All eligible individuals for whom a frozen cell sample was available were tested. I am not certain I can come up with potential biases in patient selection. Comment 12: -Statistical significance is not established by p-values, 0.05 but due to sample size selection from the population of interest using a type I error level of 0.05. Authors should correct their statement in the methods section. Response 12: I am not sure I understand this comment. To try to respond…. If we had seen no statistically significant differences it would be valuable to know that our sample size was large enough to not have missed what was there. Since here we report differences that are significant at the level of p<0.05 does that not imply that the sample size was large enough to detect the differences detected? Comment 13: -How many observations per patient were used for the analyses presented? Response 13: 1 observation per patient. Comment 14: -How authors handled missing data, specially because this is a retrospective information collected? Response 14: There was no missing data. If samples were not available for time points that met the inclusion criteria, then the time points were not included in the study. However, due to the limited amount of cells available for each time point tested, not all immune parameters could be tested for every time point. Comment 15: - Which statistical method was used for testing trends as described in the results section? Response 15: The same statisitical methods. Trends were reported for observations of interest that did not achieve a p-value of 0.05 Comment 16: -How was the sample size calculated and power used for selecting the patients for this analysis? Response 16: No sample size was calculated, essentially we studied all subjects meeting the criteria available for which frozen cells were available. Comment 17: Results: -Unclear what is IQR for these authors. If IQR represents interquartile range, it is just a number and not two numbers as the authors reported. Are they presenting minimum or maximum, quartiles? This raised major concerns in the statistical aspects of this paper. Response 17: IQR is interquartile range and as the term implies the 2 numbers represent the 25 and 75th percentile values surrounding the median. The way IQR is presented in the manuscript is consistent and accepted with current published journal articles. Comment 18: -Authors should report gender in percentages instead of absolute values Response 18: We could do this but I am not certain it is an improvement over reporting number given the small population size. Comment 19: -Unclear why, how, and where the Mann-whitney test is reported in figure 1. Response 19: Figure 1 A shows a representative plot of 1 patient each in the good and poor CD4 group. No Mann-Whitney test was reported for the data presented in Figure 1, rather a Spearmans correlation test was used to assess the strength of the association between CD4 count change and proliferation to CMV and HIV Gag p55. However, a MannWhitney test was used to compare the dichotomized results for proliferation to Gag p55 and percent CD4+CD57+ cells comparing the patients groups with good vs. poor CD4 change after treatment interruption. These results were reported in the text in the Results section but refer to a different way of looking at the results than the correlation analyses presented in Figure 1B. Comment 20: -Unclear paragraph on page 8, what are the comparison groups and the test presented for comparing what with what? Response 20: We dichotomized the 13 subjects by the median CD4+ count loss into the good vs. poor CD4 group and then we proceed to compare the various immune parameters between these two groups. This is stated in the text of the Result section. Comment 21: -What is the definition of the authors for immune predictors? Response 21: We would define an immune predictor as an immunological parameter that can be tested before stopping therapy that would have a predictive value in determining whether the patient will experience poor outcome or not after stopping therapy. Such a test could be further validated with a goal of eventually being used in clinical decision making on whether or not to stop therapy. Comment 22: Discussion: -Authors should minimize their discussion substantially for example authors claimed that their results presented “SHOWED” clear evidence for their findings, however there is not a clear population study or description that they have enough sample size for their conclusions or hypothesis of interest. Response 22: See above and we can do this Comment 23: -Author lack to motivate readers to compare their findings with other because it is impossible to know from where these patients come from to use their results, especially because authors indicate that this is key for those using “drug holidays”. Implications and links to real clinic is lacking in this version of the manuscript. Response 23: This manuscript presents results that are a first step to identifying markers that may predict outcome following treatment interruption. We are not suggesting these markers should be used in the clinic but rather that they could be explored in larger studies that would be powered to validate their use in the clinic. Comment 24: -Authors lack to evaluate all the potential biases found in their sample in terms of the epidemiological components. Response 24: This comment is vague. I don’t know what epidemiological components that the reviewer wants us to address. Comment 25: -What are the limitations of this research and your findings? Response 25: Small sample size. Comment 26; Figure 1 -Please review titles. Response 26: This can be been done Comment 27: -Are the correlations across multiple measures in time for these patients? Response 27: No, the correlations are for one measure in time within 12 months of treatment interruption. Comment 28: -What does the rectangle measures in figure 1 section A? Response 28 See response to comment 9. Comment 29: -Why are graphs presented for selected patients instead of all patients? What is the message they want to communicate to readers? Why are these contour graphs important in measuring the correlation? Response 29: See response 8… This is a standard way to show results. Figure 1A shows representative raw data and figure 1B shows all the data for measures of interest versus change in CD4 which is defined in the text as the difference between CD4 count before and after treatment interruption. Comment 30: -Why there is a different notation in this graphs and the text? What is CD4 count change??? In time??? Response 30: There is no difference in the notation between the graphs and the text. CD4 count change is the change in CD4 count between the pre-TI baseline time point to the lowest CD4 count during treatment interruption (TI). Comment 31: -It seems authors think that a not statistical significant p-value for a spearman correlation coefficient indicates lack of correlation. However, their graphs indicated that they are measuring is linearity of their correlation which is usually the case with Pearson correlation. Authors need to review what are their testing when reporting each p-value in their manuscript and figure. Response 31: The test performed was Spearman correlation. The line was added to show linearity. This is commonly done as seen in other publications. However, we could remove the line to avoid confusion with Pearson correlation as the reviewer suggested. Comment 32: -Graphs in section B do not include 13 patients, why? What the line represents in these graphs? How the assumptions for the line provided here were evaluated? -Why the correlation coefficients are different between text and figure? -When were these variables measured? Response 32: 1. 2 graphs in section B do not include 13 patients because we did not have sufficient cells to test that parameter. The line is to show the linearity. See Response 30 for further clarification. 2. The correlation coefficients are the same between the text and Figure 1. This has been verified. The only discrepancy is between the p-value in Figure 2 where it is 0.0095 in the figure but rounded up to 0.001 in the text. This could easily be corrected. 3. These variables were measured with the cells from the one pre-TI baseline time point for each patient. Comment 33: -What are the socio-demographic characteristics of these patients? Response 33: This not relevant for our study and does not influence the conclusions we draw.