Study of Serum Fibrotic Markers in Correlation with Liver Biopsy in

Non-Invasive prediction of Fibrosis in Patients with
Chronic Hepatitis C infection
Abd El-Baset MZ , Younis YS, MAGDY A. GAD , Entsar H. El-sharqawy , EL-Saiedy AZ* AND ISSA HA**
From departments of Hepatology, Gastroenterology and Infectious diseases , Pathology*,clinic pathology , Faculty of medicine, Banha University,
Abstract
Liver fibrosis due to HCV infection is a dynamic process during which different biochemical markers are released in the blood. The aim of this study was to assess non invasive markers of liver fibrosis in CHC and to correlate them with fibrosis stage assessed by liver biopsy.
Fourty six cases were subjected to estimation of tissue inhibitor of metalloproteinase 1(TIMP-1) and hyaluronic acid
(HA) by ELISA technique, scoring of the age-platelet index(API), AST to platelet ratio index(APRI), and liver biopsy with histopathological grading and staging using METAVIR scoring system. Results: There were positive correlation between age, platelet decrement with fibrosis stage. HA level increased significantly with fibrosis progression, and at cut-off 26.4 ng/ml, can be used to discriminate F>2, as detected by ROC curve, with 80% sensitivity, and 71% specificity.
TIMP-1 levels were positively correlated with METAVIR stages, and can be used as a test for F>2 discrimination with 86.7% sensitivity and 64.5% specificity. API showed a significant positive correlation with fibrosis and necroinflammation (P < 0.01), by using ROC curve for F> 2 discrimination with specificity 61.3% and sensitivity 73.3%, when API > 2.5. While APRI showed a significant positive correlation with METAVIR activity grade and stage (p < 0.01), and by using
APRI for predicton of significant fibrosis and cirrhosis F > 2, the AUC 0.89 with 93.3% and 74.2% for sensitivity and specificity respectively. Conclusion: HA level had strong positive correlation with significant fibrosis; TIMP-1 levels were positively correlated with METAVIR stage. API and
APRI showed significant strong positive correlation with METAVIR stage and activity grade.
Introduction
Hepatitis C virus (HCV) infection and its complications are known to be a major public health problem in Egypt, where 10-15% (about 9 million) of general population is infected. Approximately 20% of chronically infected patients develop
1 complications such as liver fibrosis and cirrhosis. Subsequent complications include liver failure and hepatocellular carcinoma, which are the main cause of mortality
2
(Frank et al., 2000).
Chronic HCV infection results in complicated cascade of immune mediated inflammatory events that result in inflammation, necrosis, fibrosis and cirrhosis (Duffour , 1997).
Until recently, liver fibrosis has been believed to be irreversible, but recent studies suggest that liver fibrosis and cirrhosis are a dynamic process and potentially reversible Schuppan et al.,( 2003) and Afdhal and Nunes,(
2004).
Nowadays, serum fibrotic biochemical markers that provide alternatives to liver biopsy in patients with chronic HCV, as fibro test for assessment of fibrosis and
Acti test for necroinflammatory activity are being used, (Poynard et al., 2002 and
Myers et al., 2002) , but their results don't consistently predict either the presence or absence of significant fibrosis and could not reliably be used to reduce the need of liver biopsy (Rossi et al., 2003).
Liver fibrosis due to HCV infection is a dynamic process during which different biochemical markers associated with connective tissue turnover are released into the blood for example increased serum level of procollagen III N-terminal peptide (PIII NP) (Murawaki et al., 1994) , decreased serum level of matrix metalloproteinase (MMP-1) (Murawaki et al., 1999) , associated with severe necro-inflammation, and progression of fibrosis indicated by increased levels of 7S fragment of type IV collagen (PIVNP) (Murawaki et al.,
1994) , hyalouronic acid (Patel et al.,2003) , gelatinase A (Murawaki et al., 1999) , and tissue inhibitor of metalloproteinase (Murawaki et al., 1994).
In addition, cytokines such as transforming growth factor TGFβ1 strongly up regulates production and deposition of the major extracellular matrix molecules (Gressner,
2002) .The measurement of two combined serum markers for example: PIII NP
(reflecting fibrogenesis) and MMP-1 (reflecting fibrolysis) identified cut-off values that provided reliable information about the amount of liver fibrosis in chronic HCV
(Leroy et al., 2004) .
3
AIM OF THE WORK
The aim of this study is to assess the value of serum TIMP-1 and HA as non invasive markers of liver fibrosis in chronic hepatitis C and to correlate their serum levels with the stage of fibrosis assessed by histopathological staging of liver biopsy .
PATIENTS and methods
This study was carried out on 46 patients with chronic hepatitis C, they were
(34) male (73.9%) and (12) female (26.1%).All cases were selected from the department of Hepatology Gastroenterology, and Infectious diseases, Benha
University hospitals, El Qaliobya Governorate .
Exclusion criteria were:-
1.
Subjects with active schistosomiasis.
2.
Subjects with schistosomal hepatic fibrosis grade II & III by ultrasonography.
3.
Carriers for HBV (seropostivity for HBsAg ± anti-HBc.
4.
Subjects who had received antiviral therapy.
5.
Subjects suffering from other liver diseases not related to HCV e.g. autoimmune hepatitis, sclerosing cholangitis.
Patients were subjected to the following:-
1Full history taking : especially duration of infection.
2Thorough clinical examination: especially organomegaly
3Abdominal ultrasonography:- real time abdominal sonography was done with TOSHIBA ECCOCEE machine using convex sector probe (3.5HZ).
4Rectal snip was done to exclude active schistosomaisis.
5Routine laboratory investigations including: Complete blood count,
4
liver profile tests: prothrombin time, prothrombin concentration, serum albumin, AST, ALT, alkaline phosphatase, γGT and serum Bilirubin,
viral markers: HCV-Ab & HBsAg by ELISA technique and
HCV-RNA - PCR.
6.
Assessment of serum tissue inhibitor of metalloproteinase- 1 (TIMP-1).
7.
Assessment of serum hyalouronic acid.
8.
Scoring of age- platelet index (API).
9.
Scoring of AST to platelet ratio index (APRI).
10.
Liver biopsy and histopathological examination for necroinflammatory grading and fibrosis staging applying the METAVIR scoring system.
Assessment of serum tissue inhibitor of metalloproteinase- 1 (TIMP-1): by
TIMP-1 ELISA kit is a non isotopic immunoassay for the in vitro quantitation of human TIMP-1 protein in tissue culture media and serum.
Sample collection and storage:
Serum: a serum separator tube was used and allowed blood sample to clot 30 min. once clotted, samples are centrifuged at 1000 x g for 10 min. Carefully remove serum and assay immediately or aliquot and store samples at < -20 ْ c.
Freeze/ thaw cycles were avoided.
Principle of the assay: The TIMP-1 ELISA was a "sandwich" enzyme immunoassay employing two monoclonal antibodies. A monoclonal antibody, specific for human TIMP-1 protein, had been immobilized onto the surface of the plastic wells provided in the kit. The sample was assayed (test samples and standards), were pipetted into the wells and any human TIMP-1 protein present binds to the capture antibody. Unbound material was washed away and a monoclonal, horseradish peroxidase (HRP)-conjugated anti-TIMP-1 antibody was added to the wells. Following this incubation and a wash step, a chromogenic substrate was added to the wells. The HRP catalysed the
conversion of the chromogenic substrate tetra-methelbenzidine (TMB) from a colorless solution to a blue solution (or yellow after the addition of stopping reagent), the intensity of which was proportional to the amount of human
TIMP-1 protein in the test sample. The colored reaction product was quantified using spectrophotometer.
Quantitation was achieved by the construction of a standard curve using known concentration of human TIMP-1 protein (provided lyophilized). By comparing the absorbance obtained from a sample containing an unknown amount of human TIMP-
1 protein with that obtained from the standards, the concentration of human TIMP-1 protein in the test sample could be determined.
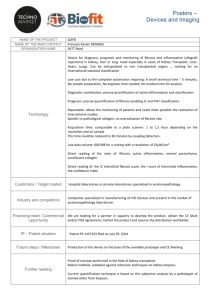
Evaluation of results: A typical standard curve generated by this kit was shown below. Data should be extrapolated from standard curves run within, and in conjugation with the test samples. A standard curve should run in duplicate each time assay was performed.
5
Fig (1): TIMP-1 ELISA (sample standard curve).
6
Assessment of serum Hyaluronic acid (HA): by hyaluronic acid test kit; using an enzyme-linked binding protein assayed for the determination of HA in the human serum or plasma .
Specimen collection and preparation: serum or heparinized plasma was the preferred sample matrices. Blood should be collected by venipuncture. Serum or plasma should be separated from cells by centrifugation. If not tested immediately, the specimens should be stored at 2-8 ْ C. if specimens were to be stored for more than 72 hours, they should be frozen at -20 ْ C or below. Specimens containing visible particulate matter should be clarified by centrifugation before testing.
- Assay procedure:
1) HA reference solutions, HA controls, and patient samples were prepared by adding 1 part of the solution or sample to 10 parts Reaction Buffer (blue solution). For example, 30 µL of sample added to 300 µL of Reaction Buffer would provide sufficient volume to test in duplicate.
2) 100 µL of diluted HA reference solutions, HA controls, patient samples and reaction buffer (for reagent blank) were added to appropriate microwells. Left the water blank well empty.
3) Incubated 60 minutes at room temperature (18- 26 ْ C).
4) After the incubation was complete, carefully invert microwells, and empty the content into a suitable container.
5) 100 µL HRP- conjugated HABP solutions (red solution) were added to all wells except the water blank.
6) Incubated for 30 minutes at room temperature.
7) After the incubation was complete, carefully inverted microwells and empty conjugate solution. Washed 4 times with PBS and tap or blot as described in step 6. Didn’t allow the wells to dry out.
8) 100 µL One- component substrate Solution was added to each well (except the water blank well) and incubated for 30 minutes at room temperature.
Added substrate solution to wells at a steady rate. Blue color would develop in wells with positive samples.
9) 100 µL Stopping Solution (0.36 N sulfuric acid) was added to each well
(except the water blank well) to stop the enzyme reaction in the same order and at the same rate as the substrate solution. Did not add stopping solution to the water blank well. Instead, added 200 µL of reagent grade water to the water blank well.
10) Blank or zero plate reader against the water blank well. The optical density
(O.D.) of each well at 450 nm (650nm reference) was read. O.D. of wells should be measured within one hour after the addition of stopping solution.
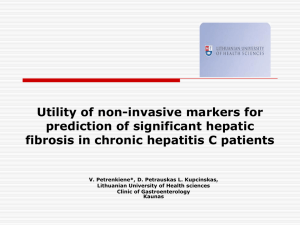
- Results:
7
Fig. (2): Hyaluronic acid Standard Curve for ELISA test.
-Normal range: serum samples from 100 healthy blood donors (population A) were tested with three HA kit lots. The mean HA value of this population was determined to be 28.5 ng/ml with a standard deviation of 24 ng/ml. A normal cut-off of 75 ng/ml was established based on the 95 th percentile of the normal population.
HA normal range = 0-75 ng/ml
Scoring the age- platelet index (API):
It is an index described by Poynard et al., (1997) as follows: Age is given scores from 0-5 as follows:
Age < or equal 30 ys is given 0 point.
Age of 31 up to 40 ys is given 1 point.
Age of 41 up to 50 ys is given 2 point.
Age of 51 up to 60 ys is given 3 point.
Age of 61 up to 70 ys is given 4 point.
Age >70 ys is given 5.
Platelets are also given scores from 0-5 as follows:-
Platelet count > and equal to 225,000/mm 3 is given 0 point.
Platelet count 200,000-224,999/mm 3 is given 1 point.
Platelet count 175,000-199,999/mm 3 is given 2 point.
Platelet count 150,000-174,999/mm 3 is given 3 point.
Platelet count 125,000-149,999/mm 3 is given 4 point.
Platelet count < 125,000 /mm 3 is given 5 point.
The simple age-platelet index was given by adding age and platelet scores, and therefore varied from 0-10.
Scoring of AST to Platelet Ratio Index (APRI):
It is an index described by Wai et al.,(2003) as follows:
APRI
AST
Platelet
Level
(
ULN
)
count
( 10
9
/
L
)
100
(Where ULN means upper limit of normal).
RESULTS
Table (1): Age and sex differences between all studied groups .
Studied variables
Age
Female
Male
F0
(no. 9)
Mean ± SD
30.4 ± 9.5
3 33.3
6 66.7
F1
(no. 13)
Mean ± SD
35.4 ± 11.6
F2
(no. 9)
Mean ± SD
42.1 ± 4.2
F3
(no. 13)
Mean ± SD
38.5 ± 8.1
3 23.1
10 76.9
4 44.4
5 55.6
2 15.4
11 84.6
F4
(no. 2 )
Mean ± SD
37 ± 7.1
0 0.0
2 100.0
Test of
Significance
ANOVA 2.1
X² test:
3.36
P- value
> 0.05
>
0.05
There is no statistical significant difference between studied groups as regards
8 age
Table (3) Studied non invasive markers andn METAVIR activity grades:
Studied variables
TIMP-1
HA
A1
(no. 33)
Mean ± SD
187.07 ± 37.8
59 ± 86.16
A2
(no. 12)
Mean ± SD
200.9 ± 44.9
116.8 ± 122.07
A3
(no. 1)
Mean ± SD
130.3 ± 0.0
50.93 ± 0.0
Test of
Significance
ANOVA test
1.66
Kruskal Wallis test
5.17
P- value
> 0.05
< 0.05
Post
Hoc test
API 2.21 ± 1.9 3.92 ± 1.3 4 ± 0.0 Kruskal Wallis test
7.75
TIMP-1 : Tissue inhibitor of metalloproteinase 1 HA : hauloronic acid API : age platelet index
< 0.05 P1>
0.05
Table (4): Relation between the disease duration in months and METAVIR stages:
Studied variables
Duration of disease in months
F0
(no. 9)
Mean ± SD
19 ± 9.7
F1
(no. 13)
Mean ± SD
43 ± 39.7
F2
(no. 9)
Mean ± SD
9.2 ± 9.4
F3
(no. 13)
Mean ± SD
32.3 ±
16.5
F4
(no. 2 )
Mean ± SD
19 ± 24.04
Test of
Significance
P- value
Kruskal
Wallis test
11.65
<0.05*
9
Table (2): Correlation of laboratory findings and METAVIR activity grades:
Studied variables
Hb
Platelets
WBCs
Albumin
A1
(no. 33)
Mean ± SD
13.64 ± 1.3
6614.2 ±
2094.6
222 ± 52.4
4.2 ± 0.51
A2
(no. 12)
Mean ± SD
13.8 ± 1.8
5510 ± 1201.3
182.9 ± 40.7
4.15 ± 0.31
A3
(no. 1)
Mean ± SD
12.6 ± 0
4700 ± 0.0
189 ± 0
2.9 ± 0.0
Test of
Significance
ANOVA test
0.31
ANOVA test
1.61
ANOVA test
2.63
ANOVA test
3.78
P- value
> 0.05
> 0.05
> 0.05
< 0.05*
Prothrombin time
13.13 ± 1.17 13.04 ± 0.79 14 ± 0.0 ANOVA test
0.35
> 0.05
Prothrombin conc
ALT
87.2 ± 12.13
80.9 ± 72
86.5 ± 7.5
65.6 ± 25.7
80 ± 0.0
24 ± 0.0
> 0.05
> 0.05
AST
Total bilirubin
Direct bilirubin
54.2 ± 42.15
0.77 ± 0.26
0.23 ± 0.14
77.5 ± 75.7
0.79 ± 0.22
0.24 ± 0.12
32 ± 0.0
0.7 ± 0
0.1 ± 0
ANOVA test
0.21
Kruskal Wallis test
1.5
Kruskal Wallis test
2.9
ANOVA
test
0.08
Kruskal Wallis test
1.87
> 0.05
> 0.05
> 0.05
Studied variables
TIMP-1
HA
Table (5): Correlation of studied non invasive markers and METAVIR stages.
F0 (no. 9)
Mean ± SD
177.2 ± 41.2
9.9 ± 6.6
F1 (no. 13)
Mean ± SD
174.14 ± 38.6
62.7 ± 88.9
F2 (no. 9)
Mean ± SD
187.8 ± 42.7
67.9 ± 98.5
F3 (no. 13)
Mean ± SD
215.3 ± 33.6
136.04 ± 118.6
F4 (no. 2 )
Mea n ±
SD
183.04 ±
19.05
5
..8 ± 16.4
Test of
Significance
Kruskal Wallis test
13.2
ANOVA test 2.26
P- value
< 0.05
< 0.05*
Post Hoc test
P1> 0.05
P2> 0.05
P3< 0.05*
P4> 0.05
P5> 0.05
P6> 0.05
P7> 0.05
P8> 0.05
P9> 0.05
P10>
0.05
API 1.9 ± 1.9 1.69 ± 1.55
APRI 0.56 ± 0.38 0.58 ± 0.35
P1 between F0 and F1
P9 between F2 and F4
1.0
3.11 ± 1.61
0.53 ± 0.04
3.61 ± 1.85
1.33 ± 0.76
5 ± 0
2.06 ±
1.51
Kruskal Wallis test
12.09
Kruskal Wallis test
18.26
< 0.05* P1> 0.05
P2> 0.05
P3> 0.05
P4< 0.05*
P5> 0.05
< 0.01** P1> 0.05
P2> 0.05
P3> 0.05
P4> 0.05
P5> 0.05
P6> 0.05
P7<
0.01**
P8> 0.05
P9> 0.05
P10>
0.05
P6> 0.05
P7> 0.05
P8<
0.05*
P9> 0.05
P10>
0.05
P2 between F0 and F2 P3 between F0 and F3 P4 between F0 and F4
P6 between F1 and F3 P7 between F1 and F4 P8 between F2 and F3
P10 between F3 and F4 APRI : AST to Platelet Ratio Index
0.8
0.6
0.4
0.2
0.0
0.0
0.2
0.8
1.0
0.4
0.6
1 - Specificity
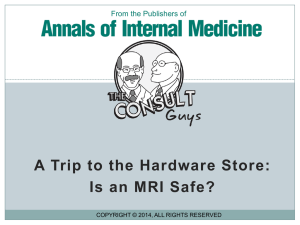
Fig (3): ROC curve testing the ability of TIMP-1 to diagnose significant fibrosis
10
Table (6): Sensitivity, specificity, area under ROC and accuracy of TIMP-1 in diagnosis of progressive fibrosis:
Studied variables Sensitivity Specificity
64.5 %
AUC
0.75
CI
75.5 % < 0.01** 0.59 – 0.9 Tissue inhibitor of
Metalloprotienase
Cut level 193.51
Accuracy P- value
1.0
0.8
0.6
0.4
0.2
0.0
0.0
0.2
0.4
0.6
0.8
1.0
1 - Specificity
Fig (4): ROC curve testing the ability of Hyalouronic acid to diagnose significant fibrosis
Table (7): Sensitivity, specificity, area under ROC and accuracy value of
Hyaluronic acid in diagnosis of progressive fibrosis:
Studied variables
Hyaluronic acid
Cut level 26.41
Sensitivity
80.0 %
Specificity
71.0 %
AUC
0.79
Accuracy P- value CI
80.1 % < 0.01** 0.66 – 0.92
Discussion
Fibrosis is a non specific response to injuries which implies the synthesis of an extracellular matrix (ECM). ECM represent a group of macromolecules, including collagens, non-collagen glycoproteins, matrix bound growth factors,
11
glycosaminoglycans, proteoglycans and matrix proteins (Friedman, 2000).
The mechanisms responsible for the fibrogenic evolution of chronic liver diseases can be summarized in 3 main groups: chronic activation of the wound healing reaction, oxidative stress-related molecular mechanisms, and derangement of the so called epithelial-mesenchymal interaction (Pinzani, 2004)
ECM is an active tissue, implying not only matrix synthesis, but also matrix degradation in a dynamic process which lead to the ECM remodeling. Thus, although fibrosis in the liver may be a progressive process leading to cirrhosis, fibrosis is also a potentially reversible process, at least in early stages (Arthur, 1998; and Arthur,
2002).
Imbalance between matrix synthesis and degradation plays a major role in hepatic fibrogenesis. Matrix degradation depends upon the balance between matrix metalloproteinases (MMPs), tissue inhibitors of MMPs (TIMPs) and converting enzymes (MT1-MMP and stromelysin) (Sherlock and Dooley, 2002) .
In the liver, stellate cells express virtually all key components required for matrix degradation. In particular, they are the key source of MMP-2, which is responsible for the degradation of type IV collagen, a major component of the basement membrane. Conversely, active MMP-2 has been shown to promote proliferation of activated stellate cells (Iredale et al; 1998 and Murawaki et al;
1997).
Hyaluronic acid (HA) is a glycosaminoglycan component of the ECM, synthesized by HSC. In normal circumstances the endothelial cells of the liver sinusoids are the site of HA uptake and degradation (Eriksson et al., 1983).
High levels of serum HA have been shown to be related not only to the stage but also to the degree of necro-inflammation ( Guechot et al., 1995 and Murawaki et al., 1995).
Histological evaluation of percutaneous liver biopsy specimens is currently used as a gold standard for assessment of hepatic fibrosis in chronic HCV infection.
However, liver biopsy carries a significant risk of pain, bleeding, biliary peritonitis
12
and pneumothorax and histological staging has several shortcomings that limit its diagnostic accuracy (Stauber and Lackner, 2007).
The assessment of fibrosis is hepatic diseases provides much information and has a high value, not only for the therapeutic decision and for the monitoring of the natural history or the evaluation under treatment (Grigorescu, 2006).
For all these considerations, several clinical studies have attempted to identify serum markers that correlate with the degree of fibrosis and thus could be used, with feasibility, in conjugation with or in place of a liver biopsy. (Wai et al., 2003;
Guechot et al., 1995 and Forns et al., 2002).
In this study, the age of patients ranged between 20-58 years, with a mean
36.7
9.4 years. There was positive correlation between age and the stage of fibrosis.
This was in agreement with many studies that showed an evidence of both continuous exposure and Cohort effects reflecting a continuing pattern of infection with different risk factors, which explained the marked rise of viral hepatitis prevalence, especially
HCV, in older ages in Egypt, and that more aggressive liver disease was detected in older patients (Abdel Wahab et al., 1994; El-Sayed et al., 1996 and Darwish et al.,
1996).
The majority of patients were males (73.9%) and this came in agreement with
Poynard et al., (2000); Abo Alazm and El Sheikh (1996) whose studies showed significant association between the male gender and fibrosis progression. Moreover,
Pinzani (2004) reported that male gender (for groups of age >50 years) has been shown to be a predictor of the development of significant fibrosis or, at least, of a faster progression to cirrhosis.
In the present study the serum albumin level significantly decreased as activity grade increased, which came in agreement with Friedman et al., 2002 who reported that hypoalbuminemia was common in chronic liver diseases.
13
In the current study, there was a statistically significant decrease in platelet count with progressive fibrosis. This result came in agreement with Sherlock and
Dooley (2002) who reported that there was a decrease in platelet count due to hypersplenism. This also explained the correlation between API and APRI with platelet count.
In the current study there was no correlation between prothrombin time (PT) and fibrosis progression, which comes in agreement with Coverdale et al., (2003) who reported that PT failed to correlate with fibrosis progression and advised not to rely upon it.On the other hand, these results disagree with Cadranel & Philippe
(2002) who found that PT was an accurate, cheap, and reproducible serum marker of extensive fibrosis .
In this study, HA level increased significantly with progression of fibrosis with good sensitivity (80%), good specificity (71%) and area under ROC (AUC
0.79). the cut-off value of HA used to discriminate significant fibrosis was 26.41 ng/ml and it was a dependant predictor factor for diagnosis of fibrosis with positive predictive value (PPV) of 57.1% and negative predictive value ( NPV) of 88%.This was supported by Halfon et al., 2005 who reported that HA was accurate in predicting significant fibrosis, severe fibrosis and cirrhosis with AUCs of 0.73, 0.77 and 0.97 respectively. Moreover, Esmat et al., 2007 used HA as optimal single test for predicting fibrosis. HA level of less than 30 ng/ml among those less than 45 years of age excluding severe fibrosis or cirrhosis with a negative predictive value of 95% and positive predictive value 45%. However, McHutchinson et al., 2000 reported that serum HA at a level of < 60 mg/L excluded significant fibrosis with a PPV
(93%) and had an important role in identification of early fibrosis, thus reducing biopsy in this subgroup of patients.Also, Wong et al., 2000 reported that HA had
(85%) sensitivity and (88%) specificity for predicting stage 4 and 5 fibrosis by modified Ishak's staging.
The current study also reveald strong positive correlation of HA with both
METAVIR grade and stage and this came in agreement with Murawaki et al., 1995
14
who reported that serum HA levels related not only to stage of fibrosis but also to degree of necro-inflammation.
In the present study, the serum levels of TIMP-1 were positively correlated with METAVIR stage and TIMP-1 detection was a useful test for discriminating cases of significant fibrosis . TIMP-1 sensitivity was 86.7% and specificity was
64.5%, (AUC 0.75) with no correlation with METAVIR activity with a PPV
(54.2%) and NPV (90.9%) at cutoff level 193.51 ng/ml.These results came in agreement with Walsh et al., 1999 who reported positive correlation with the degree of fibrosis and a striking increase in serum TIMP-1 levels were observed in the late stage of fibrosis, but not in the mild stage.In disagreement with these results, Yano et al., (1996) reported that TIMP-1 might be useful to estimate hepatic fibrogenesis associated with active inflammatory process . Lichtinghagen et al., (2000) reported alterations in circulating TIMP-1 concentrations and their correlation to inflammatory activity seemed fairly established, while their correlation to fibrosis was controversial. Chen et al., (2003) also reported that, there was significant correlation between TIMP-1 and the necro-inflammatory activity.In agreement with these results,
El-Gindy et al., (2003) reported a significant positive correlation between TIMP-1 and fibrosis stage and they recommended regular estimation of serum TIMP-1 in patients with chronic hepatitis C to assess fibrosis progression.
Leroy et al., (2004) also found a significant positive correlation between TIMP-1 level and METAVIR stage, also they found a significant positive correlation with METAVIR activity grade (which disagreed with results of this study).
Patel et al., 2004 reported that there was an algorithm including hyaluronic acid, TIMP-1, and 2 macroglobulin was shown to be effective in differentiating moderate/severe fibrosis (F2–F4) from those with no/mild fibrosis (F0–F1), although accurate delineation between stages was not possible.
The age-platelet index (API) in this study showed significant strong positive correlation with METAVIR stages and activity grades (P value < 0.01).
15
The study of ROC of API for discrimination of significant fibrosis (F> or equal
2) showed AUC (0.74) with bad specificity 61.3% and good sensitivity (73.3%) when
API > 2.5 which indicating that it was a useful test for discrimination of significant fibrosis with PPV (47.8%) and NPV (82.6%).These results came in agreement with those of Poynard and colleagues (1997) , who created this index. They reported that there was a significant positive correlation between API and necro-inflammatory activity and stage of fibrosis.Also, they reported that AUC for discrimination of significant fibrosis was (0.79
0.05) but with specificity of (93%) and sensitivity of
52% with API score > or equal to 6 which allowed a sufficient predictive value (93%) for the (57%) of the patients with significant histological features, however the NPV was not high enough to prevent a liver biopsy in patients with a lower score. The difference in results could be related to sample size, patient's criteria and different prevalence of various histological grades and stages within the studied cases.
On other hand Poynard and colleagues (1997) suggested that when API score
> or equal to 6, this enables an accurate prediction of the presence of activity and fibrosis in patients with chronic hepatitis C infection owing to its high specificity and hence the positive predictive value, so, liver biopsy could be avoided, but in patient with an index score less than 6, liver biopsy would be still mandatory because the negative predictive value was not sufficient.The results of the current study also came in agreement with those of Abd El-Baset et al., (2006) who reported that the API had a significant positive correlation with both fibrosis and necro-inflammatory activity.
Also, reported that API was a highly sensitive predictor of significant fibrosis and cirrhosis.
In the present study, the AST to platelet ratio index (APRI) showed significant positive correlation with METAVIR activity grade and stage (p value > 0.01), and by using APRI for prediction of significant fibrosis and cirrhosis (METAVIR stage > or equal 2), the AUC was (0.89) with good sensitivity 93.3% and good specificity 74.2%.These results were close to the results of Wai et al., (2003) who created this index who shown that
AUC were 0.8 and 0.89 for discriminating fibrosis and cirrhosis
16
respectively and they concluded that this index could identify significant fibrosis and cirrhosis with high degree of accuracy.Also these results came close to the results of Abd El-Baset et al., (2006) who reported that the
APRI had a significant positive correlation with both necro-inflammatory activity and fibrosis stage. Also they used APRI for prediction of significant fibrosis and cirrhosis with AUC were 0.68
0.15 and 0.69
0.15 respectively indicating a fair test. However, Romero et al., (2005) got lower figures and they reported that APRI alone could diagnose significant fibrosis in only 54% of their studied 199 patients.
In conclusion : serum HA level and TIMP-1 level were increased significantly with progression of fibrosis and also had positive strong correlation with significant fibrosis and were positively correlated with METAVIR stage .also the age-platelet index (API) and the AST to platelet ratio index (APRI) showed significant strong positive correlation with METAVIR stage and activity grades.
REFRESES
Abd El-Baset MZ, Lashin AH, Abo-Senna AA and Biomy HA (2006): Evaluation of liver fibrosis markers in chronic liver diseases". MD thesis in Banha Faculty of Medicine Results. Page
172-188.
Abdel-Wahab MF, Zakaria S, kamel M and et al., (1994): High seroprevalence of hepatitis C virus infection among risk groups in Egypt. Am. J. Trop. Med. Hyg.; 51(5):563-547.
Abo Al-Azm A and El-Sheikh M (1996): prevalence of hepatitis C and B viruses in Gharbia
Governorate rural area in comparison with a group of blood donors. JHGID; 4(4): 31-39.
Afdhal NH and Nunes D (2004): Evaluation of liver fibrosis: A concise review. Am J.
Gastroenteral. 127: 1704-1713.
Arthur MJ (2004) : Degradation of matrix proteins in liver fibrosis. Path. Res. Praact.; 190:825-832.
Arthur MJP (1998): Fibrosis and matrix degradation. Digestion; 59: 376-380.
Cadranel JF and Philippe M (2002): Prothrombin index decrease: a useful and reliable marker of extensive fibrosis. Eur. J. Gastroenterol. Hepatol.; 14(10): 1057-1059.
Chen SL and Morgan TR (2006): The natural history of hepatitis C virus (HCV) infection. Int J
Med Sci.;3(2):47-52.
17
Coverdale SA, Samarasinghe DA, Lin R and et al., (2003): Changes in antipyrine clearance and platelet count, but not conventional liver tests, correlate with fibrotic change in chronic hepatitis C: value for predicting fibrotic progression. Am. J. Gastroenterol.; 98(6): 1384-
1390.
Darwish M, Faris R, Clemens J and et al., (1996): High seroprvalence of hepatitis A, B, C and D viruses in residents in an Egyptian village in the Nile Delta. A pilot study. Am. J. Trop.
Med. Hyg.; 54(6): 554-558.
Dufiour JF, DeLellis R and Kaplan MM (1997): Reversibility of hepatic fibrosis in autoimmune hepatitis. Ann Intern Med. 1; 127(11): 981-5.
El-Gindy I, El-Rahman AT, El-Alim MA and et al., (2003): Diagnostic potential of serum matrix metalloproteinase-2 and tissue inhibitor of metalloproteinase-1 as non-invasive markers of liver fibrosis in patients with HCV- related chronic liver disease. Egypt. J. Immunol.;
10(1):27-35.
El-Sayed MN, Gomatos PJ, Rodier GR and et al., (1996): Seropervalence survey of Egyptian tourism workers for hepatitis B virus, HCV, HIV, Treponema pallidum infection: association of HCV infection with specific regions of Egypt. Am J Trop med Hyg; 55(2):
179-84.
Eriksson S, Fraser JRE, Laurent TC and et al.,(1983): Endothelial cells are a site of uptake and degradation of hyaluronic acid in the liver. Exp Cell Res ; 144: 223-228.
Esmat G, Metwally M, Zalata KR and et al., (2007) : Evaluation of serum biomarkers of fibrosis and ingmy in Egyptian patients with chronic hepatitis C. J. Hepatol; 46(4): 620-7.
Forns X, Ampurdanés S, Llovet JM and et al., (2002) : Identification of chronic hepatitis C patients without hepatic fibrosis by a simple predictive model. Hepatology. 36(4pt 1): 986-92.
Friedman LS, Mantin P and Munoz SJ (2002): Laboratory methods for evalution of the patients with liver disease. In Zakim D, Boyer TD eds. Hepatology: A textbook of liver disease,
Ithedn. Philadelphia: Samders 661-708.
Friedman SL (2003) : Liver fibrosis- from bench to bedside. J. Hepatol.; 38: S38-S53.
Frank C, Mohamed MK, Strickland GT and et al., (2000): The role of parenteral antischistosomal therapy in the spread of hepatitis C virus in Egypt. Lancet, 355(9207): 887-91.
Gressner AM, Weiskirchen R, Breitkopf K and Dooley S (2002): Roles of TGF-beta in hepatic fibrosis. Front Biosci, 7:2247-50.
18
Grigorescu M (2006) : Non-invasive biochemical markers of liver fibrosis. J Gastrointest. Liver
Dis.; 15(2): 149-59.
G uechot J, Loria A, Sefaty L and et al., (1995): Serum hyalunonan as a marker of liver fibrosis in chronic hepatitis C: effect of alpha-interferon therapy. J Hepatol, 22:22-26.
Guha N and Iredale JP (2007): Clinical and diagnostic as peer, of Cirrhosis. Page 619-634.
Textbook of hepatology "from basic science to clinical practice". 3 rd
Edition.
Halfon P, Bourliere M, Pénaranda G. and et al., (2005): Accuracy of hyalurolnic acid level for predicting liver fibrosis stager in patients with chronic hepatitis C. Comp. Hepatol. 4: 6.
Iredale JP, Murhy G, Hembry RM and et al (1992): Human hepatic lipocytes synthesize tissue inhibitor of metalloproteinase 1. Implications for regulation of matrix degradation in liver. J
Clin Invest 1992; 90: 282-287.
Iredale JP, Benyon RC, Pickering J and et al. (1998): Mechanisms of spontaneous resolution of rat liver fibrosis. Hepatic stellate cell apoptosis and reduced hepatic expression of metalloproteinase inhibitors. J Clin Invest ; 102(3):538-549.
Leroy V, Monier F, Bottari S and et al., (2004): Circulating matrix metalloproteinases 1, 2, 9 and their inhibitors TIMP-1 and TIMP-2 as serum markers of liver fibrosis in paitents with chronic hepatitis C: comparison with PIIINP and hyaluronic acid. Am J Gastroenterol,
99(2):271-9.
Lichtinghagen R, Huegel O, Seifert T and et al., (2000): Expression of matrix metalloproteinase-2 and metalloproteinase-9 and their inhibitors in peripheral blood cells of patients with chronic hepatitis C. Clin. Chemistry; 46:183-192.
McHutchinson JG, Blau LM, DeMedina M and et al.(2000): Measurement of serum hyaluronic acid in patients with chronic hepatitis C and its relationship to liver histology. Consensus
Interferon Study Group. J Gastroenterol Hepatol; 15: 945-951.
Murawaki Y, Ikuta Y, Idobe Y and Kawasaki H (1999): Serum matrix metalloproteinase-1 in patients with chronic viral hepatitis. J. Gastroenterol Hepatol, 14: 138-45.
Murawaki Y, Ikuta Y, Koda M and Kawasaki H (1994): Serum type III procollagen peptide, type
IV collagen 7S domain, central triplehelix of type IV collagen and tissue inhibitor of
19
metalloproteinases in patients with chronic viral liver disease: relationship to liver histology.
Hepatology, 20:780-7.
Murawaki Y, Ikuta Y, Nishimura Y and et al.(1995): Serum markers for connective tissue turnover in patients with chronic hepatitis B and chronic hepatitis C: a comparative analysis. J
Hepatol ; 23: 145-152.
Myers RP, Ratziu V, Imbert-Bismut F and et al., (2002): Biochemical markers of liver fibrosis: a comparison with historical features in patients with chronic hepatitis C. Am J Gastroenterol,
97:2419-25.
Patel K, Gordon SC, Jacobson I and et al.(2004): Evaluation of a panel of non-invasive serum markers to differentiate mild from moderate-to-advanced liver fibrosis in chronic hepatitis C patients. J Hepatol ; 41 :935–42.
Patel K, Lajoie A, Heaton S and et al., (2003): Clinical use of hyaluronic acid as a predictor of fibrosis change in hepatitis C. J Gastroenterol Hepatol, 18(3): 253-7.
Pinzani M (2004): Pathogenesis of hepatic fibrosis (p. 121-129). In liver Disease from bench to bedside. American Association for the study of liver disease. Massachusetts, October 29-30.
Poynard T, Imbert-Bismut F, Ratziu V and et al., (2002): Biochemical markers of liver fiborsis in patients infected by Hepatitis C virus: Longitudinal validation in a randomized trial. J Viral
Hepat., 9:128-133.
Poynard T, Bedossa P , METAVIR and CLINIVIR cooperative study groups (1997): Age and platelet count: a simple index for predicting the presence of histological lesions in patients with antibodies to hepatitis C virus. J. Viral Hepatitis; 4(3): 199-208.
Rossi E, Adams L, Prins A and et al., (2003): Validation of the Fibro Test biochemical markers score in assessing liver fibrosis in hepatitis C patients. Clin Chem, 49(3):450-4.
Schuppan D, Krebs A, Bauer M and Hahn EG. (2003): Hepatitis C and liver fibrosis. Cell Death
Differ, 10(Suppl l):S59-67.
Sherlock S and Dooley J (2002) : Anatomy and function; Biopsy of the liver and hepatic cirrhosis.
In Diseases of the liver and Biliary system "11th Edition", Blackwell Sc. Publ., Oxford,
London, Edinburgh, (1): 1-16; (3): 37-44 and (21): 365-377.
Stavbier RE and Lackner C (2007): Non-invasive diagnosis of hepatic fibrosis in chron in hepatitis
C. World J. of Gastroenterology: 13(32): 4287-4294.
20
Wai C, Greenson JK, Fontana RJ and et al., (2003) : A simple non-invasive index can predict both significant fibrosis and cirrhosis in patients with chronic hepatitis C. Hepatology; 38: 518-
526.
Walsh KM, Timms P, Campbell S and et al., (1999): Plasma levels of matrix metalloproteinase-2
(MMP-2) and tissue inhibitors of metalloproteinase-1 and-2 (TIMP-1 and TIMP-2) as noninvasive markers of liver disease in chronic hepatitis C. Comparison using ROC analysis. Dig Dis Sci; 44: 624-630.
Wong JB and Koff RS (2000) : Watchful waiting with periodic liver biopsy versus immediate empirical therapy for histologically mild chronic hepatitis C. A cost-effectiveness analysis.
Ann. Inern. Med.; 133: 665-675.
Yano M, Kumada H, Kage M and et al., (1996) : The long term pathological evaluation of chronic hepatitis C. Hepatology; 23:1334-40.
21