Diabetes Emergency Plan FINAL
advertisement

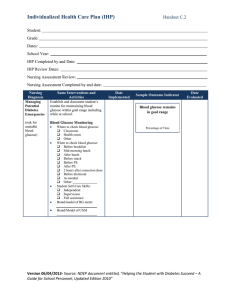
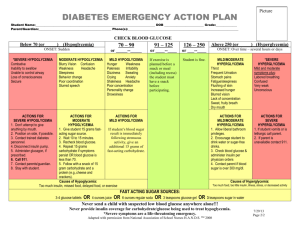
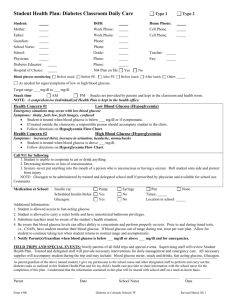
Diabetes Emergency Plan Student’s Name: ____________________________ D.O.B. ____________ Student’s Photo School: _________________ Grade: _____ Div: _____ Date of Plan: __________________ PHN Care Card Number # _______________________________________ Yes No Nursing Support Services Diabetes Delegated Care Plan NSS Coordinator: ____________________________ Phone: __________________ CONTACT INFORMATION Parent/Guardian 1: Name: Phone Numbers: Cell Parent/Guardian 2: Name: Phone Numbers: Cell: Other/Emergency: Name: Call First Work Cell: Other Call First Work: Home: Other: Relationship: Able to advise on diabetes care: Phone Numbers: Home Yes No Work: Home: Other: Additional times to contact Parent/Guardian (In addition to times indicated in NSS Delegated Care Plan): Have emergency supplies been provided in the event of a natural disaster? Yes No If yes, location of emergency supply of insulin: _____________________________________ Page 1 of 2 TREATING MILD TO MODERATE HYPOGLYCEMIA STUDENT’S USUAL SYMPTOMS OF MILD TO MODERATE HYPOGLYCEMIA Shaky, sweaty Hungry Pale Dizzy Mood changes Irritable Tired/sleepy Blurry/double vision Difficulty concentrating Confused Poor coordination Difficulty speaking Headache Other symptoms: If mild to moderate hypoglycemia is suspected, DO NOT leave student unattended TREATMENT FOR STUDENTS NEEDING ASSISTANCE (anyone can give glucose to a student): Location of fast acting sugar: ____________________________ 1. If student able to swallow, give one of the following fast acting sugars based on student’s weight: 10 grams ____ glucose tablets 1/2 cup of juice or regular soft drink OR 15 grams ____ glucose tablets 3/4 cup of juice or regular soft drink 10 mL (2 teaspoons) or 2 15 mL (1 tablespoon) or 3 packets of table sugar dissolved in water 2 teaspoons of honey packets of table sugar dissolved in water 1 tablespoon of honey 10 skittles Other (ONLY if 10 grams are 15 skittles Other (ONLY if 15 grams are labelled on package): __________________________ labelled on package): __________________________ 2. Contact designated emergency school staff person 3. Blood glucose should be retested in 15 minutes. Retreat as above if symptoms do not improve or if blood glucose remains below 4mmol/L 4. Do not leave student unattended until blood glucose is over 4 mmol/L 5. Give an extra snack such as cheese and crackers if the planned meal/snack is not for another 45 minutes or more TREATING SEVERE HYPOGLYCEMIA SYMPTOMS OF SEVERE HYPOGLYCEMIA: SEIZURE, UNCONSCIOUSNESS School staff persons trained to give glucagon: ________________________________________________ ________________________________________________________________________________________________ Location of Glucagon kit: __________________________________________________________________________ Glucagon dose: _____ 0.5 mg (5 years old or less) _______1 mg (6 years or older) Response: Do NOT try to give anything by mouth Identify someone to call 911 immediately Identify someone to call the student’s parent/guardian Turn the student on his/her side and keep them in that position until student is alert Administer glucagon in the outer thigh as per training and instructions in kit Stay with student until ambulance arrives Once student is alert and able to swallow, give juice or fast acting sugar After fast acting sugar, if the ambulance or parent has not yet arrived, give longer acting carbohydrate such as cheese and crackers if next meal is more than 30 - 45 minutes away. Other examples include granola bars, power bars, peanut butter and crackers. Parent/Guardian Signatures: Name: _________________________________ Signature: _____________________________ Date: _____________ Page 2 of 2