Hypertension Briefing for Mersey Primary Care Strategic

Paper 8a
Hypertension Briefing for Mersey Primary Care Strategic Forum
1. Introduction
Hypertension is remarkably common in the UK and the prevalence is strongly influenced by age.
It is one of the most important preventable causes of premature morbidity and mortality and is a major risk factor for ischaemic and haemorrhagic stroke, myocardial infarction, heart failure, chronic kidney disease, cognitive decline and premature death. Untreated hypertension is usually associated with a progressive rise in blood pressure.
It is one of the three main modifiable risk factors for cardiovascular disease, which account for 80% of all cases of premature coronary heart disease (CHD) (1) . Hypertension is the second biggest risk factor in the burden of disease, measured in disability adjusted life years (DALY) in the UK (2010 data) contributing to 9% of the UK DALY burden (second only to tobacco) (2) .
There is clear evidence that reduction in blood pressure is effective at reducing the risk of stroke and ischemic heart disease. Studies have shown that a reduction in blood pressure of 20 mmHg systolic or 10 mmHg diastolic is associated with reductions in death from stroke and ischemic heart disease of up to one half in those aged between 40 and 89. The findings were similar for men and women, for different types of stroke and consistent across the range of blood pressure (down to
115/75 mmHg). Reductions in usual diastolic blood pressure of 5, 7.5 and 10 mmHg were associated with reductions in stroke of 34%, 46% and 56% and coronary heart disease of 21%,
29% and 37% respectively (1) . Furthermore, the numbers needed to treat to prevent one death are very low. It is estimated that in patients with stage 1 hypertension (systolic blood pressure 140-
159mmHg and/or diastolic blood pressure 90-99mmHg) and additional cardiovascular risk factors, achieving a sustained 12 mmHg reduction in systolic over 10 years will prevent:
1 death for every 11 patients treated.
In the presence of CVD or target organ damage, only 9 patients would require such BP reduction to prevent a death (3) .
2. Local burden (Qof data)
Hypertension is the biggest QoF register, in 2012/13, 14.8% of adults were on the QoF hypertensive register in Cheshire and Merseyside (187,521 people in Merseyside). In Merseyside, the number of people on the hypertension register is rising by approximately 3000 people a year.
The expected prevalence of hypertension in Merseyside is 324,582 suggesting there could be as many as 137,061 with undiagnosed hypertension. There appears to be variation between GP practices in identifying hypertension. For example, in Knowsley, registered prevalence ranges from 12% to19.9% (expected range 21% to 29.6%).
3. Local intelligence
The QoF quality target (150/90) for hypertension differs from the NICE recommended target
(140/90) for younger patients. Local Qof data (2012/13) shows that for those who are diagnosed
1
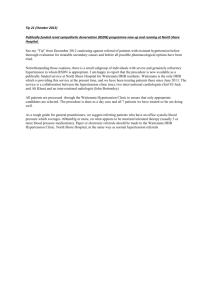
and on a register, 78% of people in Merseyside are achieving the QoF treatment target of 150/90 or less (see chart on page 2).
However, a serial Cross-sectional study (Health Survey for England) found that of those being treated for hypertension, 78% achieved 150/90 mm Hg, whereas 37% achieved 140/90 mm Hg (4) .
350 000
300 000
250 000
200 000
150 000
100 000
50 000
Diagnosis and management of Hypertension across
Merseyside
324 582 187 521 168 835 146 444
-
Modelled Prevalence of Hypertension
Diagnosed
Prevalence of
Hypertension
BP04 - Record of blood pressure measurement in previous 9mths
BP05 - Blood pressure in previous
9mths 150/90 or less
4. Impact on health services
The diagnosis, treatment and follow-up of patients with hypertension is one of the most common interventions in primary care, accounting for approximately 12% of primary care consultation episodes in 2006 (1).
The North of England Hypertension Guideline Development Group, which developed the NICE guideline for hypertension, estimated that, in England alone, the cost of drugs used for lowering blood pressure is £840 million per year – almost 15% of the total annual cost of drugs in primary care (5).
According to the Department of Health (2013) (6) , 45% of hypertension remains undiagnosed until an acute event occurs. Substantial savings are therefore realised as case finding for this undiagnosed cohort increases. Even though prescribing and management savings reduce as case finding increases, the savings in secondary care are much greater as the number of acute events reduces. The commissioning for value pack for CVD across Merseyside suggests there are
£830,000 opportunity costs that could be saved by reducing CVD related hospital admissions (7) .
A recent report from Essex found that improving case finding by approximately 10% would result in
£386,000 of net savings in the first year, and £1,668,000 over three years, due to reductions in secondary care admissions for stroke, vascular dementia and ischaemic heart disease (11) .
The report also calculated monetary net savings of approximately £300 for every £1 invested by the CCG in terms of costs.
5. System-wide action:
2
The make a real dent in this huge burden of disease, effort needs to be corralled from multiple partners in a systematic way (See Appendix A). The following are examples of what can be done within primary care alone:
5.1 IDENTIFYING THE MISSING 137,000.
Workings together to promote NHS Health Checks – 2012/13 data for Merseyside shows that 54,514 people (16%) were invited for the NHS Health Check; 4% short of the 20% national target. Of those invited, uptake varied between local authorities from
29% to 54%, with the average being 47% (25,471were seen in total). There is still some way to go before we reach the Public Health England (PHE) uptake target of
70%. According to the Ready Reckoner Tool (8) on current performance, 959 additional people were prescribed and compliant with anti-hypertensive medication, where as if uptake was increased to 70% this would increase to 1492 (533 additional people).
Targeted NHS Health Checks – There may also be an opportunity to target NHS
Health Checks using computer searches to identify those who; have a high CVD risk, or have a number of known risk factors, or those who we do not have risk factor data on as they have not have attended primary care for a number of years.
Bench marking and searches of practice records – e.g. searching for patients with more than one high blood pressure reading without a diagnosis and therefore not on register, or those who have had a borderline high blood pressure but not attended for follow-up/diagnosis.
Other opportunistic interventions – There are a range of other interventions that could be used. For example blood pressure monitors in practice reception areas; targeting other at risk groups e.g. diabetics, COPD; funding pharmacy outreach and or a public campaign. Stockport CCG, supported by Stockport Council is running a campaign to promote awareness of the health risks of hypertension and the importance of having blood pressure checked regularly. As well as promotional activities, they have installed wellbeing Kiosks (8)
5.2 OPTIMISING MANAGEMENT
Audit of current management against NICE quality standards - this could be undertaken by working with Informatics Merseyside and setting up a task and finish group, with clinical and public health representation, to design an audit and benchmarking tool. An audit could also look at optimal, cost effective prescribing
(against NICE and the local formulary). Work in Essex (10) has shown potential cost savings of applying NICE guidance to prescribing. The audit of current management of hypertension in primary care could be used to identify and prioritise potential interventions e.g. development of Merseyside guidance, training, consideration of models of care provision (e.g. hypertension clinics and facilitated access to lifestyle services).
3
We may be able to secure bespoke advise/support to do a ‘deep dive’ from the
Commissioning for Value/Right Care Team.
Consider prioritising those with CVD risk of 20% or more - There is evidence using
Numbers Needed to Treat (NNT) data that targeting interventions at those with hypertension and additional CVD risk factors (such as smoking, obesity, and cholesterol) may bring five year NNT down from 321 to 16 (9).
Developing locally agreed quality standards which reflect outcomes e.g. impact on patients of reaching target BP, resulting impact on end organ damage, MI, stroke, heart failure.
Develop a local network approach - For example, Tower Hamlets developed local networks of clinicians, provided project support and they were incentivised in that they got paid if ALL practices achieved the target. Key CVD indicators improved faster in
Tower Hamlets than in England, or London, and in 2012/13, Tower Hamlets ranked top in QOF for blood pressure and cholesterol control in coronary heart disease (CHD) and diabetes. Also, male mortality from CHD was fourth highest in England in 2008 and reduced more than any other PCT in the next 3 years; reducing by 43%.
References
1. NICE QS28, March 2013, Quality Standard for hypertension. http://www.nice.org.uk/Guidance/QS28
2. Murray et all, March 2013. UK health performance: findings of the Global Burden of Disease Study
2010. Lancet 2013; 381: 997 –1020
3. National Heart, Lung, and Blood Institute (US); August 2004. The Seventh Report of the Joint
National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. http://www.ncbi.nlm.nih.gov/books/NBK9626/
4. Falaschetti et all, May 2014. Hypertension management in England: a serial cross-sectional study from 1994 to 2011. Lancet 2014: 383: 1912-19
5. Faculty of Public Health (2005), Easing the Pressure: Tackling Hypertension - A toolkit for developing a local strategy to tackle high blood pressure.
6. DH Cardiovascular Disease Team, March 2013, Cardiovascular Disease Outcomes Strategy,
Gateway reference 18747, Department of Health, London. Public Health England,(May 2014) CVD
Commissioning for Value Focus Packs 2013/14. www.gov.uk/phe www.ncvin.org.uk
7. http://www.stockporthomes.org/main.cfm?Type=NI&objectid=3701
8. Wallis et al 2002. Cardiovascular and coronary risk estimation in hypertension management. Heart
2002;88:306 –312
9. World Health Organisation, 2013. A global brief on hypertension, World Health Day 2013.
WHO/DCO/WHD/2013.2
4
10. Wake, I (2013). Preventing Stroke and Ischaemic Heart Disease through Improving Case Finding of
Hypertension and Clinical Management of Hypertension and CHD in Basildon and Brentwood CCG.
[Report] Basildon and Brentwood Clinical Commissioning Group . April 2013.
July 2014 ,Sarah McNulty, Ruth du Plessis, Chris Williamson, Andrew Lui and Ifeoma Onyia
Appendix A: System wide action
Organisation
Primary Care –
General Practice
Potential Actions
• Improve uptake of NHS health checks (including BP)
• Active case finding e.g. search records for unregistered patients, partially diagnosed
• Opportunistic testing – e.g. flu clinics, other LTC reviews
• Audit of management against quality standards
• Audit of prescribing and prescribing guidance
• QSG topic for primary care
Primary Care
Clinical
–
Commissioning
Groups
• Prioritise hypertension (Identification and treatment)
• Develop and resource a local hypertension pathway
• Work with local acute trusts in pathway development
• Explore variation (prevalence & outcomes) at GP practice level
• Review current prescribing against NICE guidelines
NHS England
Local Authorities/ /
Health and
Wellbeing Boards
Public Health
England
Strategic Clinical
Networks
The third sector
Other partners
• Agree local targets and quality standards
• Staff training
• Make it a Health & Wellbeing Board priority across Merseyside
• Action on primary prevention i.e., salt levels in food, obesity prevention – for example, influence local planning, lobby industry
• Commissioning NHS Health Checks to ensure reach and appropriate follow up, consider targeted approaches
• Working with partners to promote Health Checks
• Directors of Public Health, (collaborative service) promote though healthy places agenda and collective action
• Use SLI process with LGA
• Use Overview and Scrutiny process – there are mechanisms for cross-LA processes to be set up
• Engage PHE as key partners in the work programme on hypertension
• Include hypertension as a priority area for public campaigns – e.g. ‘Know
Your Number’
• Gain support from SCN as part of the CVD network’s programme of work
• Discuss support to improve quality
• Stroke association – Know your BP events
• British Heart Foundation - research and campaigns such as ‘Move
More’
• Discuss merits of having BP monitors more readily available – e.g. GP surgeries
• Health Watch
• Academic institutions
• Pharmacists, Opticians, Dentists
5
• Acute Trusts esp. LHC
• Chamber of Commerce & local industries
• Public Sector organisations
6