Contents - Vula - University of Cape Town
advertisement

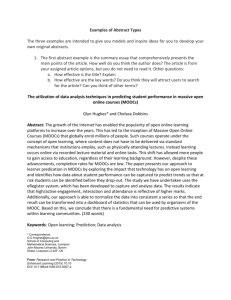
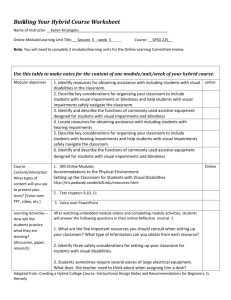
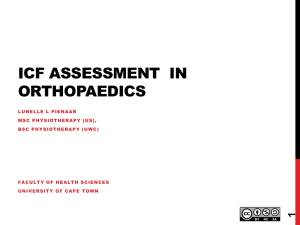
Approach to Assessment AHS2050H J Jelsma Clinical Physiotherapy I - AHS2050H Module on Assessment Jennifer Jelsma 2010 1 Approach to Assessment AHS2050H J Jelsma Contents: Contents: ............................................................................................................... 2 Programme: ............................................................. Error! Bookmark not defined. Objectives: ............................................................................................................ 3 Introduction: .......................................................................................................... 3 ICF Model .............................................................................................................. 5 Details of components ....................................................................................... 6 Impairments of body functions and structures ............................................. 6 Activity limitations and participation restrictions ......................................... 6 Environmental factors .................................................................................... 6 Personal factors ............................................................................................. 7 Outline of approach to assessment ...................................................................... 7 Demographic and medical history..................................................................... 7 Interview (subjective)........................................................................................ 7 Objective (examination) .................................................................................... 8 Analysis .............................................................................................................. 8 Examples of how the framework can be used: ................................................ 9 Problem List..................................................................................................... 12 Short term aims ............................................................................................... 12 Long term aim .................................................................................................. 12 SOAP Notes ..................................................................................................... 12 Task..................................................................................................................... 13 Case study; ...................................................................................................... 13 Guidelines for assessment of children with neurological damage or developmental delay ........................................................................................... 14 1. Demographic details .................................................................................... 14 From folder: .................................................................................................. 14 2. Subjective assessment ................................................................................ 15 Impairments (only describe impairments relevant to the individual child) 15 Activities ....................................................................................................... 15 Participation .................................................................................................. 15 Environment .................................................................................................. 15 3. General Observation.................................................................................... 15 How did child get to physiotherapy department? ....................................... 15 4. Objective Assessment ................................................................................. 16 a. Activity ...................................................................................................... 16 b. Impairments ................................................. Error! Bookmark not defined. 5. Problem List ................................................................................................ 17 6. Short term aims ........................................................................................... 18 7. Long term aim.............................................................................................. 18 8. SOAP Notes ................................................................................................. 18 2 Approach to Assessment AHS2050H J Jelsma Objectives: At the conclusion of the module, the student should be able to: Describe the rehabilitation cycle Describe the components of the International Functioning, Disability and Health. (ICF) Classification of Describe the process of patient assessment Explain how the ICF philosophy can be used as a framework to collect and analyse patient data and to decide on treatment priorities. Introduction: One of the most difficult skills that a physiotherapy student has to learn is clinical reasoning. In order to meet the needs of a patient, the student needs to know what the needs are, analyse these needs and the problems that are causing them, choose and apply suitable techniques and then assess whether the intervention has been effective. There have been several models of the clinical process that have been developed, but the most common model is a cyclical model in which assessment leads to appropriate treatment which then leads to changes in the condition of the patient. These changes need to be assessed and the cycle begins once more. An example of the rehabilitation cycle is given below1 1 Steiner WA, Ryser L, Huber E, et al. Use of the ICF Model as a clinical problem-solving tool in physical therapy and rehabilitation medicine. Phys Ther 2002; 82: 1098-1107 3 Approach to Assessment AHS2050H J Jelsma Figure 1. The Rehab-Cycle is a modified version of the Rehabilitation Cycle developed by Stucki and Sangha.14 It guides the health care professional with a logical sequence of activities. Endpoints of this rehabilitation management system are successful problem solving or individual goals achieved. The Rehab-CYCLE involves identifying the patient’s problems and needs, relating the problems to relevant factors of the person and the environment, defining therapy goals, planning and implementing the interventions, and assessing the effects. (Reprinted with permission of the American Physical Therapy Association. Figures may be used for educational purposes, research purposes, or personal use. Commercial use is prohibited.) The problem is that there is so much information that must be gathered. Some of it is not important and some ends up by being essential. The inexperienced clinician needs to learn how to gather all relevant data, but also not to waste time by gathering information that has no bearing on the planning of the patient’s management. How do we go about gathering this information and how do we go about analysing the information to decide on treatment goals and intervention? A useful framework to manage the information gained during patient assessment is the ICF (International Classification of Functioning, Disability and Health)2. This is a system of classification which helps users to identify the different aspects of a person’s condition that can impact on health and 2 World Health Organization. International Classification of Functioning, Disability and Health. Geneva: World Health Organization; 2001. 4 Approach to Assessment AHS2050H J Jelsma functioning. It can be used to gather information in a standardised manner through the use of codes. It is also possible to use the philosophical framework to gather information and plan treatment. The ICF has different components: Impairments of body structure (eye) and function (seeing) Activity limitations (rolling, walking, dressing) Participation restrictions (limited access to education, transport) Environmental factors: (policies such as education policy for disabled children, physical environment, availability of aids, appliances) ICF Model The first models of disability were linear. In other words, the problem with the person (handicap) was a direct result of the injury. Disease or disorder Impairments Disabilities Handicaps As time went on, it became clear that disability was far more complex and the ICF presented the following model: Interaction of Concepts ICF 2001 Health Condition (disorder/disease) Body Function & structure (Impairment) Environmental Factors Activities (Limitation) Participation (Restriction) Personal Factors Based on World Health Organization (2001) International classification of functioning, disability and health: ICF. Geneva: World Health Organization, pg. 18. Accessed online: http://www.disabilitaincifre.it/documenti/ICF_18.pdf 5 Approach to Assessment AHS2050H J Jelsma Details of components Impairments of body functions and structures Functions Mental functions Sensory functions (including pain) Voice and speech functions Functions of the cardiovascular, haematological, immunological and respiratory systems Functions of the digestive, metabolic and endocrine systems Genitourinary and reproductive functions Neuromusculoskeletal and movement related functions Functions of the skin and related structures Structures Structures of the nervous system Eye, ear, related structures Structures involved in voice and speech Structures of the cardiovascular, haematological, immunological and respiratory systems Structures related to the digestive, metabolic and endocrine systems Structures related to the genitourinary and reproductive systems Structures related to movement Skin and related structures Activity limitations and participation restrictions Learning &Applying Knowledge General Tasks and Demands Communication Movement Self Care Domestic Life Areas Interpersonal Interactions Major Life Areas Community, Social & Civic Life Environmental factors Products and technology Natural environment and human-made changes to the environment Support and relationships Attitudes Services, systems and policies 6 Approach to Assessment AHS2050H J Jelsma Personal factors These are not coded by the ICF but include behaviours specific to the individual, such as smoking or enthusiasm about the treatment programme. Outline of approach to assessment Demographic and medical history Interview (subjective) Impairments - only ask about impairments relevant to the individual and his/her condition o Mental, function o Communication o Sensory (sight, pain, sensation) o Cardiovascular o Digestive, feeding, continence, sexual function o Neuromuscular o Skin condition Activity limitations: o Learning and applying knowledge o Communication o Mobility: o Hand use and lifting and carrying objects o In bed: rolling, bed pan use, reaching locker, shifting in bed o Sitting o Standing o Walking o Self-care: o Washing, toileting, dressing, eating o Physical activity (highest level of activity, duration or distance?) Participation o Interpersonal relationships: strangers, family and friends o Play, education, work, o Recreation and leisure – community life sport, participation in religion Environmental factors: o Aids, appliances, wheelchairs o Support and attitudes of others o Housing: Accessibility, adaptions o Transport 7 Approach to Assessment AHS2050H J Jelsma o Social services (e.g. grants) Objective (examination) This is planned based on the subjective interview and only those impairments and activities which have been identified as problems are assessed. This part of the assessment is more specific to the health condition of the patient. E.g. thorough examination of respiratory function is essential in a patient with asthma, but not necessary in an NMS patient. In addition, special measurements and tests must be included. E.g. goniometry for impairments of the neuromuscular system or the AIMS to determine the activity limitations of children. The order of assessment can be the same as the subjective, but not always. For example, in a patient whose main problem is pain, it is likely that the pain and the neuromuscular will be assessed first, whereas in children with CP, the highest level of physical functioning is usually assessed. Analysis Once the information has been gathered, the clinician needs to make sense of what he/she has found. What are the patient’s main problems? (These are usually activity limitations or participation restrictions, but not always. Pain or productive coughing are examples of impairments that could be the main problems) What are the underlying causes of these problems? (These are usually impairments, e.g. weak muscles, soft tissue damage, pain in the knee on walking) How can change in either impairments or activity limitations be measured The ICF can help to identify patterns and to analyse the relationships between the different findings. In addition, it can help the clinician to prioritise the problems that the patient needs to have addressed first. 8 Approach to Assessment AHS2050H J Jelsma Examples of how the framework can be used: Health Condition Activities Participation Body Functions and Structures Home Environment Personal Figure. Relationships among components of functioning, environmental, and personal factors that were important for Teresa at 17 months of age (represented by thick lines). Based on Physical Therapy, Volume 86, Number 9, September 2006. A collaborative model of service delivery for children with movement disorders: a framework for evidence-based decision making, by RJ Palisano. Health Condition Body Functions and Structures Home Environment Activities Participation Personal Figure. Relationships among components of functioning, environmental, and personal factors that were important for Teresa at 17 months of age (represented by thick lines). Based on From: Physical Therapy, Volume 86, Number 9, September 2006. A collaborative model of service delivery for children with movement disorders: a framework for evidence-based decision making, by RJ Palisano. 9 Approach to Assessment AHS2050H J Jelsma Note how the same child’s problems change as she gets older. View Stucki G, Ewert T, Cieza (A. Value and application of the ICF in rehabilitation medicine. DisabilRehabil 2002; 24: 932-938, figure 2) for an example of using the structure in a patient with back pathology. The difference between the patients and the therapists perception and analysis of the problems is highlighted. See Steiner et al., Use of the ICF Model as a clinical problem-solving tool in physical therapy and rehabilitation medicine, 2002; 82:1098-1107, figure 4, available here:http://ptjournal.net/content/82/11/1098/F4.expansion.html) for an example of using the ICF to analyse the problems of a patient with chronic pain. It does not matter exactly which schema is used for analysis, as long as all components are considered. It is suggested that the original model be used, as in the example below, applied to a patient with a fracture of the tibia/fibula in the early stages of treatment. 10 Approach to Assessment AHS2050H J Jelsma HEALTH CONDITION Fractured tib/femur acute. Car accident.External fixation IMPAIRMENTS ACTIVITY LIMITATION PARTICIPATION RESTRICTION Pain in thigh Soft tissue damage Weak muscles quads and gluts Limited RoM of knee Swelling Sore under heel Bed rest Unable to look after infant at home Lost domestic work job due to accident Productive cough Anxious Cannot bridge to use bed pan Cannot shift in bed Cannot reach locker Cannot come into sitting No balance in standing ENVIRONMENTAL FACTORS PERSONAL FACTORS Locker not close to bed No husband Supportive mother Ward has no parallel bars Home - one story and accessible to wheelchair and crutch walking Not yet applied to Road Accident Fund for compensation Overweight Depressed Smoker How would the priorities change if the patient were to be discharged in the next day or so? 11 Approach to Assessment AHS2050H J Jelsma Problem List Once the analysis has been done, the most important FUNCTIONAL problems should be identified and documents Prioritise the most important problems and analyse completely, using the following table. Functional Problems Usually activity or participation (but could be pain or respiratory function) Missing Components If necessary for movement analysis Underlying reasons Usually impairments of body function Intervention indicator Either for impairments (e.g. pain VAS) or activities (e.g. AIMS) Short term aims Must be functional aims (likely to be achieved in the next few treatment sessions) Long term aim Think of ONE function you would like to improve in 6 months’ time. SOAP Notes Includes daily updates on the Subjective, Objective, Analysis of Problems (SOAP) and treatment plan. 12 Approach to Assessment AHS2050H J Jelsma Task Read through case study Identify what problems the patient has and what codes could be used to describe his/her condition using ICF checklist Refer to ICF diagram and identify which domains are most problematic for the patient Using the diagram, identify which domains are connected and in what way. Finally write your problem list with underlying causes, based on the interactions noted in the ICF Diagram. Case study; Sophie is a 2 year old child who has Tuberculosis. She started on treatment two months ago. She is an in-patient at Brooklyn Chest Hospital because her mother is very ill with HIV and her grandmother is caring for three other children. Her father is in jail. It is therefore unlikely that she will receive her medication regularly. She is a withdrawn child who rarely smiles. She does not say very much and does not seem to understand English at all. She does not play with toys and generally is quite apathetic.. She has an itchy rash on her stomach which irritates her and causes her to scratch. She has a productive cough and easily gets short of breath. She has problems with keeping her medication down and often vomits during treatment. She is kept in nappies by the nursing staff. She is undernourished and small for her age. She has weak trunk muscles and her muscle tone is decreased. She has no limitation of range of movement. She is able to roll and come into sitting. She crawls a little and can pull up into standing. However, she is unable to walk independently. She is likely to stay in hospital for the next three months. 13 Approach to Assessment AHS2050H J Jelsma Guidelines for assessment of children with neurological damage or developmental delay ICF FRAMEWORK Health Condition (disorder) Body function & structure Activities Participation Environmental Personal Factors Factors Based on World Health Organization (2001) International classification of functioning, disability and health: ICF. Geneva: World Health Organization, pg. 18. Accessed online: http://www.disabilitaincifre.it/documenti/ICF_18.pdf Note in which area the child is experiencing the most problems. What are the connections between these elements? 1. Demographic details NAME: DATE OF BIRTH: ASSESSMENT: AGE: DIAGNOSIS: ASSESSED BY: DATE OF From folder: BIRTH HISTORY SUBSEQUENT HISTORY MEDICATION – type and what it is for 14 Approach to Assessment AHS2050H J Jelsma SURGERY – date and type 2. Subjective assessment Impairments (only describe impairments relevant to the individual child) Mental function Sight, hearing Speech Feeding Pain Respiratory or cardiac function Continence Skin condition Activities Learning and applying knowledge Communication Self-care; dressing, bathing, brushing teeth Physical activity (highest level of activity, duration or distance?) Participation Domestic life (how he spends his day?) Interpersonal relationships Community and social life Environment Appliances Transport Accessibility in home (type of house, no. of rooms, no. of people sleeping per room, available amenities, space move around) and other areas Support of community and family involvement Services (disability and child support grant) 3. General Observation How did child get to physiotherapy department? Is child walking, in a buggy or wheelchair, using appliances? 15 Approach to Assessment AHS2050H J Jelsma Observe child undressing and comment 4. Objective Assessment a. Activity START AT HIGHEST FUNCTIONAL LEVEL! If standing, assess POSTURE in standing, with appliances on. If in a wheelchair, assess POSTURE in wheelchair (this is where he spends most of his time) Describe and analyse FUNCTION IN HIGHEST LEVEL. If ambulant, describe walking Running Jumping Hopping left and right Stair climbing Throwing and catching a ball Assess BALANCE in highest functional level, both static and dynamic. Observe and describe how child moves to a lower functional level, e.g. Transitional movement from STANDING TO SITTING ON A CHAIR AND STANDING TO SITTING ON THE FLOOR AND BACK UP AGAIN. Observe and describe how child gets into and out of HALF KNEELING, KNEELING and CRAWLING. Is child able to maintain these positions? Is he able to play in these positions? Describe type of play. If the highest functional position is SITTING SUPPORTED IN A WHEELCHAIR, describe what child can do in this position. Can he reach and grasp an object? Can he hold a pen and write? Does he need help in getting out of wheelchair – how much assistance does he need? Transfer child to the mat. Can he SIT UNSUPPORTED? If not, describe what is preventing him from doing so. Try LONG SIT, CROSS LEG SITTING, SIDE SITTING. What can he do in these positions, eg. maintain position with bilateral arm support, free one hand to reach or play, move out of these positions? 16 Approach to Assessment AHS2050H J Jelsma If child is unable to sit, position him in SUPINE. Describe function in this position. Can he reach symmetrically with both arms? Can he kick legs? Can he roll to SIDE LYING or PRONE? In PRONE describe what he can do. Describe how he gets into PUPPY PRONE, can he maintain this? Can he lift his head? Can he free one arm and reach forward without collapsing on opposite side? Can he creep in this position, describe how. Can he move out of this position into SUPINE or CRAWLING POSITION? Describe this movement. b. Impairments RESPIRATORY CONDITION TONE Describe tone in all affected muscle groups. ROM If full range of motion, document FROM. If range is limited, you must measure limitation with goniometer and record accurately. MUSCLE LENGTH AND STRENGTH Note when muscle is shortened. 4. Review ICF Framework before analysing problems 5. Problem List Document FUNCTIONAL problems Prioritise the most important problems and analyse completely, using the following table. Functional Problems Usually activity or participation (but could be pain or respiratory function) Missing Components If necessary for movement analysis Underlying reasons Usually impairments of body function Intervention indicator Either for impairments (e.g. pain VAS) or activities (e.g. AIMS) 17 Approach to Assessment AHS2050H J Jelsma 6. Short term aims Must be functional aims (likely to be achieved in the next few treatment sessions) 7. Long term aim Think of ONE function you would like to improve in 6 months time. 8. SOAP Notes Including progress and any changes you need to make to your intervention plan 18 Approach to Assessment AHS2050H J Jelsma Clinical Physiotherapy: Approach to Assessment (AH2050H) by Jennifer Jelsma, Physiotherapy Division, Department of Health and Rehabilitation Sciences, University of Cape Town (2010) is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 2.5 South Africa License. Please see http://creativecommons.org/licenses/by-nc-sa/2.5/za/ for terms and conditions. All images created by external parties retain their original licenses Source work available at vula.uct.ac.za Permissions beyond the scope of this license may be available at www.healthedu.uct.ac.za or healthoer@uct.ac.za 19