Hypertension community clinic referral form (june 2013)
advertisement
")
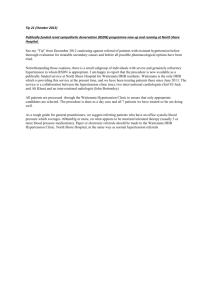
HYPERTENSION COMMUNITY CLINIC REFERRAL FORM Email your referral to gst-tr.KHPCommunityAF@nhs.net Referral date: Patient Details Title Surname First Name Address Referrer Details (Stamp) NHS Number: Is an interpreter required? Y/N If so, which language? Date of Birth Age Gender Ethnicity Telephone (Home/mobile/work) MANDATORY INFORMATION Patient needs transport please? Y/N (Incomplete form will be returned) Blood tests: Urinalysis (dipstick): Protein: Blood: Glucose: (incl. dates or provide a record extract) Creatinine: eGFR: Urine ACR: Glucose: HbA1c: CVD risk (JBS2): % Date: TSH: (T4:) Urate: ECG (Recent within last 12 months, please attach) ☐ ALT/SGPT: (GGT:) TC: HDL-C: TG: Past Medical History, ALL Current medication(s) & BP reading history: please provide a medical record extract PAST antihypertensive medications (this information is most important, please be as accurate as possible) Name Dose Reason stopped WHY ARE YOU REFFERING THIS PATIENT? (See referral guidance for inappropriate referrals) Y/N Please give any relevant details Resistant hypertension (>3 antihypertensives) Multiple adverse reactions to antihypertensive therapies Persistent non-adherence to drug therapies despite primary care team best efforts Patients in whom prescribing decisions are complex due to co-morbidities (e.g. CKD & ACE/ARBs) If NO to all of the above questions, please detail why would you like your patient to be seen? Please ensure the following have been addressed prior to referral BP measurement is accurate Lifestyle advice given Drugs which increase BP have been stopped SLCSN treatment algorithm has been followed Adherence issues have been addressed Associated conditions have been addressed? (Obstructive Sleep apnoea, obesity & insulin resistance) Y/N Accurate technique & cuff size? Arrhythmia excluded by manual pulse palpation? Diet, salt intake, physical activity, weight loos, alcohol moderation, smoking E.g.: NSAIDs, oral contraceptive pill & ciclosporine. Especially check OTC medications! http://www.slcsn.nhs.uk/files/prescribing/hypertensi on-012012.pdf Ask patient & check issues and quantities Simplify & optimize drug regimen, discuss / use dosette box If this referral is not accepted for the hypertension pharmacist community clinic would you be happy for this referral to be considered for a consultant lead hypertension clinic? Y/N HYPERTENSION COMMUNITY CLINIC - Referral guidance Referral criteria – definitions: Resistant hypertension: defined as BP not controlled despite 3 drugs at max dose or max tolerated dose. Pseudo hypertension in the elderly: o Overestimation of BP by sphygmomanometer measurement due to arteriosclerosis and/or calcification in arteries. o When to suspect: Absence of end-organ effects in long-standing "hypertension" Treatment-resistant hypertension Development of hypotensive symptoms on medications Calcification of brachial artery on radiological examination Palpable radial artery pulse despite an upper arm inflated cuff occluding the brachial artery When to suspect secondary hypertension? Suspect a secondary cause resistant treatment, BP increasing for no reason after being well controlled, and/or severe onset. Hypertension: whoif to refertoand where? 1. 2. Renal artery stenosis: o In young resistant to treatment hypertension o Deteriorating renal functionService: with ACE/ARBs inhibitors, especially in patient with PVD Community Hypertension o Abdominal bruit Resistant hypertension (defined as BP not controlled despite 3 drugs at maximum dose or maximum tolerated dose) Phaeochromocytoma: anxiety,topostural hypotension, headaches, palpitations, pallor, excessive sweating. Multiple adverse reactions antihypertensive therapies Conn's syndrome: hypokalaemia with increased or normal sodium. Patients in whom prescribing decisions are complex dueplasma to co-morbidities Cushing: truncal obesity, moon face, purple striae, muscle weakness, easyGP bruising, Persistent non-adherence to drug therapies despite best efforts of the practicehirsutism, hyperglycaemia, hyperlipidaemia. To note, the community clinic will also undertake follow up of specific patients reviewed in secondary care specialist Gynaecomastia: can be seen patients with chronic renalfor failure, andcare. adrenal hyperplasia tumors. But do hypertension services and in discharged withhyperthyroidism, a management plan suitable primary exclude drug-induced gynaecomastia (amphetamines, calcium antagonists, anabolic steroids, cyclosporine methyldopa, angiotensin-converting-enzyme (ACE) inhibitors, and alpha-1 blockers). Secondary care specialist services o Emergency referral (A&E) Accelerated or malignant hypertension (BP>180/110mmHg), especially if evidence of grade III-IV retinopathy (papilloedema / retinal haemorrhages) Suspected TIA Suspected Aortic dissection o Hypertension clinic: Suspected secondary hypertension: Phaeochromocytoma, Coon's syndrome, Cushing syndrome, Diagnosed obstructive sleep apnoea syndrome, Rapidly worsening hypertension, Hypertension in young individuals (<40 years) especially with no FH of hypertension & where a secondary cause is suspected. Labile hypertension Pseudo-hypertension in the elderly o Other relevant services: o Renal: renal disease, renal artery stenosis o Obs & Gynae: hypertension in pregnancy o Fall clinic: postural hypotension after exclusion of common causes