Treatment Type I Open Fractures in Pediatrics (PROOF)
advertisement
")
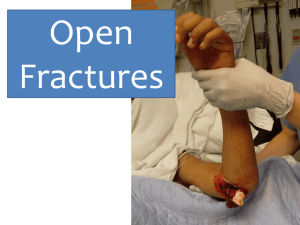
Phoenix Children’s Hospital Research Institute (PCRI) Website Clinical Trial Listing ** Please complete and return to Shy Walker at swalker@phoenixchildrens.com Study Title: The Treatment of Type I Open Fractures in Pediatrics (PROOF) Study Purpose (2-3 sentences in laymen terms): Open fractures are frequently encountered in orthopaedics. Treatment usually calls for a formal, operative procedure in which the bone is exposed, foreign tissue is debrided and the wound is irrigated. While this is the current standard of care, not all open fractures are equal. In retrospective studies, centers are reporting less aggressive operative management for open fractures may result in equal results without the time and expense of the operative theater. The investigators propose a prospective, randomized trial of children with type I open fractures to evaluate whether formal operative treatment is necessary. The investigators' hypothesis is that minor open fractures can be safely treated in the emergency room with irrigation, closed reduction and home antibiotics without an increased risk of infection or other complications. Children who meet the study criteria will be randomized into two treatment arms - formal operative management (OR) and emergency department (ED) management. Outcomes from each group will be evaluated and compared, including rate of infection, number of return visits to the operating room, time to union, and other complications. Study Summary (1 paragraph in laymen terms): Fractures in which bone has been exposed to the outside world through an associated skin injury, known as open fractures, are frequently encountered in orthopaedics. Traditionally, treatment calls for a formal, operative treatment in which the bone is exposed, foreign tissue is debrided and the wound is irrigated. The bone itself, depending on the age of the patient, fracture location and stability is then treated by the appropriate method of casting or internal fixation. However, while this is the current standard of care for all open fractures, not all open fractures are the same and can differ in terms of the bone involved, energy causing the injury and the skeletal maturity of the patient. Children, for example, have a thick periosteum which may diminish the rate of infection and decrease the time to healing. In addition, the protocol of operative debridement was introduced at the same time as widespread antibiotic use. It is not known whether the mechanical operative management or antibiotic use has resulted in improved outcomes. In retrospective studies, centers are reporting emergency department management alone may result in equal results without the time and expense of the operative theater. We propose a prospective, randomized trial of children with type I open fractures to evaluate whether formal operative treatment is necessary. Our hypothesis is that minor open fractures in children can be safely treated in the emergency room with irrigation, closed reduction and home antibiotics without an increased risk of infection or other complications. If the inclusion criteria is met and informed consent is obtained, children will be randomized into two treatment arms - formal operative management (OR) and emergency department (ED) management. Children randomized to the OR arm will be taken to the OR within 24 hours for irrigation and debridement and appropriate bone management. Children in the ED arm will have a washout in the emergency room under conscious sedation, a closed reduction and home antibiotics. Both wounds will be examined at interval follow up periods for signs of infection. Outcomes evaluated will include the rate of infection, the number of return visits to the operating room, the time to bone healing, and other complications. This is a pilot study with the plan of eventually being a multicenter study evaluating open fracture care in children. Basic Eligibility Criteria (1 paragraph in laymen terms): Ages Eligible for Study: 3 Years to 14 Years Inclusion Criteria: open fracture amenable to treatment by closed reduction low energy mechanism of injury (e.g., falls from less than 10 feet, bicycle accidents) wound less than 1cm in length and the bone not visualized through the skin Exclusion Criteria: open fracture not amenable to treatment by closed reduction open fracture that would typically require operative reduction and fixation high energy mechanism of injury (e.g., struck by vehicle, motor vehicle accidents, fall from height greater than 10 feet) wound greater than 1cm in length gross contamination of wound open fractures involving hands or feet (the current standard of care to treat open injuries involving hands or feet is only emergency room management) Study Location(s): Phoenix Children’s Hospital Study Contact(s): Carla Boan, MSc cboan@phoenixchildrens.com