Coding Rules - Current as at 16-Mar

Australian Consortium for Classification Development
Ref No: Q2694 | Published On: 15-Mar-2015 | Status: Current
ACCD Classification Information Portal
SUBJECT: Total parenteral nutrition (TPN)
For New Zealand the advice for TPN is effective for events with an event date on or after 1 July 2015
Q:
Should total parenteral nutrition be coded?
A:
Total parenteral nutrition (TPN) is the administration of nutrients to a patient usually via a central venous catheter and is usually a short term treatment, although in some conditions has been used as a long term therapy.
TPN is classified in ACHI under Pharmacotherapy and the guidelines in ACS 0042 Procedures not normally
coded, point 8 should be followed:
8. Drug treatment/pharmacotherapy
Drug treatment should not be coded except if:
• the substance is given as the principal treatment in same-day episodes of care
• drug treatment is specifically addressed in a coding standard (see ACS 0044 Chemotherapy, ACS 1316
Cement spacer/beads and ACS 1615 Specific interventions for the sick neonate).
(Coding Rules, March 2015)
Coding Rules - Current as at 16-Mar-2015 05:02 Page 1 of 28
Australian Consortium for Classification Development
Ref No: Q2820 | Published On: 15-Mar-2015 | Status: Current
SUBJECT: Cellulitis of an infected blister
ACCD Classification Information Portal
Q:
Patient admitted for cellulitis of an infected blister of the index finger. Swabs taken of the blister grew
Staphylococcus aureus which clinical documentation confirmed as the source of the infection. Should a code for cellulitis be assigned as well as T79.3 Post traumatic wound infection, not elsewhere classified, as per ACS 1916 Superficial injuries?
A:
ACS 1916 Superficial injuries instructs that T79.3 Post traumatic wound infection, not elsewhere classified and a code for the associated infectious agent should be assigned as additional codes if a superficial injury is infected. The instruction in the specialty standard should be followed despite T79.3 being an NEC code. However it does not preclude the assignment of a more specific code for the infection, such as cellulitis in the scenario cited.
For example:
Patient admitted for cellulitis of an infected blister of the index finger. Documentation in the clinical record confirms an associated infection with Staphylococcus aureus.
The following codes would be assigned (and sequenced following the principles in ACS 0001 Principal
diagnosis):
L03.01 Cellulitis of finger
S60.82 Blister of wrist and hand
T79.3 Post traumatic wound infection, not elsewhere classified
B95.6 Staphylococcus aureus as the cause of diseases classified to other chapters and appropriate external cause of injury codes.
ACS 1916 Superficial injuries has been identified for review for a future edition.
(Coding Rules, March 2015)
Coding Rules - Current as at 16-Mar-2015 05:02 Page 2 of 28
Australian Consortium for Classification Development
Ref No: Q2853 | Published On: 15-Mar-2015 | Status: Current
ACCD Classification Information Portal
SUBJECT: Increased S/D (systolic/diastolic ratio) and AEDF (absent end diastolic flow)
Q:
What code should be assigned when increased S/D (systolic/diastolic ratio) or AEDF (absent end diastolic flow) is documented as a reason for induction of labour or caesarean section?
A:
Both systolic/diastolic blood flow velocity ratio (S/D ratio) and end diastolic flow (EDF) are measurements of umbilical artery blood flow in the Doppler ultrasound assessment. Many studies have come to the conclusion that increased S/D and absent end diastolic flow (AEDF) are useful markers in detecting at risk fetuses and in predicting placental insufficiencies.
Assign O36.5 Maternal care for poor fetal growth for documentation of increased S/D or AEDF as it includes maternal care for known or suspected placenta insufficiency. This is the usual indication for intervention such as induction of labour or elective caesarean section.
Improvement to ICD-10-AM will be considered for a future edition.
(Coding Rules, March 2015)
Coding Rules - Current as at 16-Mar-2015 05:02 Page 3 of 28
Australian Consortium for Classification Development
Ref No: Q2862 | Published On: 15-Mar-2015 | Status: Current
ACCD Classification Information Portal
SUBJECT: Invasive and in-situ neoplasms of the prostate
Q:
If a trans-rectal ultrasound (TRUS) guided biopsy of the prostate identifies adenocarcinoma (M8140/3) and high grade intraepithelial neoplasia (M8148/2), do you code both or just the adenocarcinoma?
A:
Where a histopathology report details both in situ and invasive cancer within the prostate, the behaviour takes precedence over the histological type and only the morphology and site code for the invasive cancer should be coded.
The sentence in ACS 0233 Morphology:
“If a morphological diagnosis contains two histological terms which have different M codes, select the
highest number as it is usually more specific.” is referring to multiple histological types found within a lesion in one organ, and does not provide guidance with respect to differing morphological behaviours.
In the scenario cited where multiple histological terms/morphologies with different behaviours are reported in a TRUS biopsy of the prostate, only assign codes for the invasive neoplasm (i.e. adenocarcinoma).
This will be clarified in ACS 0233 Morphology in a future edition.
(Coding Rules, March 2015)
Coding Rules - Current as at 16-Mar-2015 05:02 Page 4 of 28
Australian Consortium for Classification Development
Ref No: Q2872 | Published On: 15-Mar-2015 | Status: Current
ACCD Classification Information Portal
SUBJECT: Gastroenteritis or diarrhoea due to Norovirus
Q:
What is the correct code assignment for gastroenteritis or diarrhoea due to Norovirus?
A:
Norovirus was previously referred to as “Norwalk-like viruses”, Norwalk viruses, and small round-structured viruses.
The World Health Organization (WHO) provides the following definition in the ICD-11 Beta version:
The official genus name Noroviruses which is the group of viruses previously described as “Norwalk-like viruses” are a group of related, single-stranded RNA, non-enveloped viruses. Noroviruses cause self-limiting explosive acute gastroenteritis that last for 24-48hours in humans. The most common symptoms of acute gastroenteritis are diarrhea, vomiting, and stomach pain (WHO, 2015).
Therefore intestinal infections due to norovirus should be assigned A08.1 Acute gastroenteropathy due to
Norwalk agent, following the index pathway:
Gastroenteritis
- viral
- - Norwalk agent A08.1
Diarrhoea caused by norovirus should also be assigned A08.1 Acute gastroenteropathy due to Norwalk agent, following the index pathway:
Diarrhoea, diarrhoeal
- due to
- - virus (see also Enteritis/viral) and
Enteritis
- viral
- - small round structured A08.1
Improvements to the Alphabetic Index with respect to norovirus will be considered for a future edition of
ICD-10-AM.
Reference:
World Health Organization (WHO) (2015). ICD-11 Beta version, joint linearization for mortality and morbidity statistics. Retrieved from http://apps.who.int/classifications/icd11/browse/l-m/en
(Coding Rules, March 2015)
Coding Rules - Current as at 16-Mar-2015 05:02 Page 5 of 28
Australian Consortium for Classification Development
Ref No: Q2874 | Published On: 15-Mar-2015 | Status: Current
ACCD Classification Information Portal
SUBJECT: Interpretation of ACS 0936 Cardiac and implanted defibrillators
Q:
What is the correct interpretation of the following sentences in ACS 0936 Cardiac pacemakers and
implanted defibrillators regarding the classification of insertion of electrode(s) for implanted cardioverter defibrillators (ICDs)?
“The code(s) should be assigned based on the type of electrode (pacemaker or defibrillator) and the route
(transvenous, epicardial etc) regardless of how, or if, they are subsequently used.”
“Where an electrode has both pacing and defibrillating functionality, apply the hierarchy and assign
defibrillator electrode code(s) only.”
A:
Most modern implanted cardioverter defibrilIators (ICDs) have the functions of both pacing and defibrillation as rate-responsive bradycardia pacing is now standard in all ICDs. Some types of ICDs only have one electrode (lead) which has both pacing and defibrillating functionality while others have multiple electrodes with the additional of a pacemaker electrode that can sense the atrial electrical activity.
For initial insertion of an ICD with single electrode, assign a code for the ICD generator and a code for a defibrillator electrode only as per the hierarchy specified in ACS 0936 Cardiac pacemakers and implanted
defibrillators. For example, initial insertion of a single chamber ICD with an electrode positioned in the right ventricle via transvenous route, assign:
38393-00 [653] Insertion of cardiac defibrillator generator and
38390-02 [648] Insertion of permanent transvenous electrode into other heart chamber(s) for
cardiac defibrillator
For initial insertion of an ICD that has multiple electrodes, assign a code for the ICD generator and codes for each type of electrode (not device/generator). For example, initial insertion of a dual chamber ICD with one defibrillator lead fixed in the right ventricle and an additional pacemaker lead fixed in the right atrium via transvenous route, assign:
38393-00 [653] Insertion of cardiac defibrillator generator and
38390-02 [648] Insertion of permanent transvenous electrode into other heart chamber(s) for
cardiac defibrillator and
38350-00 [648] Insertion of permanent transvenous electrode into other heart chamber(s) for
cardiac pacemaker
To assist with the correct code assignment for insertion of ICDs, review the documentation in the clinical record as to both the functionality and location of the electrode(s). In the absence of documentation of this information, assign the default code 38390-02 [648] Insertion of permanent transvenous electrode into
other heart chamber(s) for cardiac defibrillator, by following the ACHI Alphabetic Index:
Coding Rules - Current as at 16-Mar-2015 05:02 Page 6 of 28
Australian Consortium for Classification Development
Insertion
- electrode(s) lead(s)
- - cardiac (for)
- - - defibrillator (automatic)
- - - - permanent
- - - - - transvenous (atrium) (right ventricle) 38390-02 [ 648 ]
ACCD Classification Information Portal
Assign an additional code 38390-01 [648] Insertion of permanent transvenous electrode into left ventricle
for cardiac defibrillator for insertion of an electrode into left ventricle if it is for a biventricular defibrillator.
Improvements to this area of classification will be considered for a future edition.
Reference:
Bänsch, D., Schneider, R., Akin, I. Nienaber, C. A. (2015). A New Single Chamber Implantable Defibrillator with Atrial Sensing: A
Practical Demonstration of Sensing and Ease of Implantation. Retrieved from http://www.jove.com/video/3750/a-new-singlechamber-implantable-defibrillator-with-atrial-sensing
Rüdiger, K.; Klaus-Peter; H. Robert, P. S. (2012). Defibrillators and ICD systems. Springer Handbook of Medical Technology.
(Coding Rules, March 2015)
Coding Rules - Current as at 16-Mar-2015 05:02 Page 7 of 28
Australian Consortium for Classification Development
Ref No: Q2876 | Published On: 15-Mar-2015 | Status: Current
SUBJECT: Total femur replacement
ACCD Classification Information Portal
Q:
How do you code total femur resection with reconstruction including total femur replacement?
A:
Total femur replacement is a rare procedure, alternatively known as:
• Total femur endoprosthetic replacement
• Endoprosthetic femoral replacement
• Total femoral endoprosthetic reconstruction
• Total femur arthroplasty
• Total femur resection, and reconstruction with total femur replacement.
The last dot point above most accurately describes the intervention; resection of the whole femur with joint reconstruction, and replacement of the femur using metallic endoprosthesis.This procedure was originally performed for primary bone and soft tissue sarcomas, as a limb preservation/salvage procedure, an alternative to amputation.
More recently, indications have included:
• Multiple failed total hip or total knee arthropathies
• Chronic infections or other complications following multiple open reductions with internal fixation
(ORIF) of the femur
• Complex periprosthetic fractures not amenable to other treatments.
Total femur replacement is considered for the above indications when patients have insufficient residual bone to support implantation of a revision arthroplasty prosthesis or fixation device. The procedure may require extensive soft tissue dissection (including detachment of relevant muscles) and reconstruction of the joints above and below (ie knee and hip).
ACHI contains a code for this procedure, created when the procedure was primarily performed for primary bone and soft tissue sarcomas. However, regardless of the indication for the procedure, assign the following code for total femur replacement (or any of its synonymous terms):
50218-03 [1570] En bloc resection of lesion of long bone of lower limb with replacement of adjacent joint.
The indication for the procedure will be identified by the assignment of an appropriate ICD-10-AM code.
Amendments will be considered for a future edition of ACHI.
(Coding Rules, March 2015)
Coding Rules - Current as at 16-Mar-2015 05:02 Page 8 of 28
Australian Consortium for Classification Development
Ref No: Q2880 | Published On: 15-Mar-2015 | Status: Current
SUBJECT: Debridement of skin with suturing
ACCD Classification Information Portal
Q:
Is it necessary to assign a code for suturing of skin in addition to a code for (excisional) debridement?
A:
When excisional debridement is performed, it is not necessary to assign an additional code for suturing of a wound at the same site of the debridement. The suturing of the wound is a component of the procedure, as per the guidelines in ACS 0016 General Procedure Guidelines/Procedure components.
Improvements to ACHI Alphabetic Index will be considered for a future edition.
(Coding Rules, March 2015)
Coding Rules - Current as at 16-Mar-2015 05:02 Page 9 of 28
Australian Consortium for Classification Development
Ref No: Q2882 | Published On: 15-Mar-2015 | Status: Current
ACCD Classification Information Portal
SUBJECT: Thrombectomy and embolectomy of multiple arteries
Q:
Should site specific procedure codes for thrombectomy/embolectomy be assigned when thrombectomy/embolectomy is performed on multiple vessels or does the second dot point of Point 2
Multiple procedures in ACS 0020 Bilateral/multiple procedures apply?
A:
Site specific procedure codes should be assigned when thrombectomies/embolectomies are performed on multiple vessels as the procedures are performed on different lesion, for example thrombus of tibial artery and thrombus of femoral artery. The second dot point of Point 2 Multiple procedures in ACS 0020
Bilateral/multiple procedures which states ‘embolisation of left and right uterine arteries’ applies to treating the same condition/lesion which is uterine fibroid.
Q:
What is the correct code to assign thrombectomy/embolectomy of one artery and stent of another for atherosclerosis?
A:
A code for insertion of stent should be assigned in addition to the thrombectomy/embolectomy code in this scenario as two different conditions/lesions; thrombus/embolus of one artery and atherosclerosis of another artery were treated. The includes note ‘that with stenting’ at block [702] Arterial embolectomy or
thrombectomy only applies if the stenting is performed to the same artery.
Q:
Should a code for percutaneous transluminal balloon angioplasty (PTA) with stent be assigned in addition to the thrombectomy/embolectomy code when a grafted artery has thrombectomy/embolectomy and PTA stenting performed as there is no includes note at block [703] Embolectomy or thrombectomy of an arterial
bypass graft?
A:
A separate code for insertion of stent is not required if a grafted artery has thrombectomy/ embolectomy and stenting performed as per the nonessential modifier ‘with stenting’ in the following index pathways:
Embolectomy
- artery (with stenting)
- - femoral 33806-09 [702]
- - - bypass 33806-12 [703]
- - iliac 33806-08 [702]
- - - bypass 33803-02 [703]
- - innominate 33803-01 [702]
- - - bypass 33803-02 [703]
- - intracranial NEC 90235-00 [702]
- - mesenteric 33806-05 [702]
- - - bypass 33803-02 [703]
- - popliteal 33806-10 [702]
- - - bypass 33806-12 [703] or
Coding Rules - Current as at 16-Mar-2015 05:02 Page 10 of 28
Australian Consortium for Classification Development
Thrombectomy
- artery (with stenting)
- - femoral 33806-09 [702]
- - - bypass 33806-12 [703]
- - iliac 33806-08 [702]
- - - bypass 33803-02 [703]
- - innominate 33803-01 [702]
- - - bypass 33803-02 [703]
- - intracranial NEC 90235-00 [702]
- - mesenteric 33806-05 [702]
- - - bypass 33803-02 [703]
- - popliteal 33806-10 [702]
- - - bypass 33806-12 [703]
ACCD Classification Information Portal
An additional code for PTA from block [754] is not required as PTA is inherent in the stenting procedure.
Improvements to ACHI will be considered for a future edition.
(Coding Rules, March 2015)
Coding Rules - Current as at 16-Mar-2015 05:02 Page 11 of 28
Australian Consortium for Classification Development
Ref No: Q2886 | Published On: 15-Mar-2015 | Status: Current
SUBJECT: Skin rollering
ACCD Classification Information Portal
Q:
What is the correct procedure code to assign for skin rollering?
A:
Skin rollering is also known as skin needling or percutaneous collagen induction therapy. A dermaroller with tiny stainless steel acupuncture needles causes multiple tiny pinpoint puncture wounds to the dermis. This dermal damage induces the production of new collagen and elastin, resulting in smooth skin, soft lines and reduction of stretch mark and scars through the skin’s natural wound healing process. Skin rollering creates damage to the dermis but without the removal of the healthy epidermis, which happens with other resurfacing techniques.
As there is no specific ACHI code for skin rollering procedure, assign:
90676-00 [ 1660 ] Other procedures on skin and subcutaneous tissue following the index pathway:
Procedure
- skin (subcutaneous tissue) NEC 90676-00 [ 1660 ]
(Coding Rules, March 2015)
Coding Rules - Current as at 16-Mar-2015 05:02 Page 12 of 28
Australian Consortium for Classification Development ACCD Classification Information Portal
Ref No: Q2887 | Published On: 15-Mar-2015 | Status: Current | Status: Updated 15 December 2015
SUBJECT: E13 Other specified diabetes mellitus
Q:
Can you assign multiple codes when documentation indicates that a patient has type 2 diabetes mellitus
AND diabetes mellitus classifiable to E13?
A:
ICD-10-AM classifies diabetes mellitus to the following categories:
E10 Type 1 diabetes mellitus
E11 Type 2 diabetes mellitus
E13 Other specified diabetes mellitus
E14 Unspecified diabetes mellitus
E13 Other specified diabetes mellitus cannot be assigned in addition to E10 Type 1 diabetes mellitus or
E11 Type 2 diabetes mellitus, as these codes are mutually exclusive.
E13.- is assigned by following the index pathway Diabetes/specified NEC. The NEC (not elsewhere classified) indicates that if the diabetes is classifiable to a specified category (E10 or E11), that category takes precedence over the ‘other’ (residual) category (E13).
Therefore, E13 should never be assigned when documentation confirms diabetes mellitus as type 1 or type
2.
See Conventions used in the Alphabetic Index of Diseases/NEC.
Documentation issues
The above advice is applicable to cases where type 1 or type 2 diabetes mellitus are correctly identified and documented in the clinical record.
Clinicians may incorrectly document the type of diabetes and/or use terms interchangeably, especially in relation to insulin use. For example:
• patient with type 2 diabetes mellitus (T2DM) on insulin, incorrectly documented as IDDM (insulin dependent diabetes mellitus) or type 1 diabetes mellitus (T1DM)
• patient with T2DM on insulin, inconsistently documented as T1DM or T2DM within the one episode
• patient with diabetes mellitus due to a specified cause treated with insulin, incorrectly documented as T1DM or IDDM.
The following should be noted:
• IDDM and NIDDM (noninsulin dependent diabetes mellitus) are outdated terminology
• IDDM and NIDDM are not types of diabetes; they are descriptors of insulin usage
• IDDM does not always mean T1DM; it may mean T2DM treated with insulin or DM due to a specified cause (eg post pancreatectomy) treated with insulin.
Where documentation is conflicting or inconsistent within the current episode regarding the type of diabetes mellitus, coders should check previous admissions and/or correspondence and/or consult with the treating clinician to determine if the patient has T1DM, T2DM or diabetes mellitus due to a specified cause
(meaning not type 1 or type 2).
See also ACS 0401 Diabetes mellitus and intermediate hyperglycaemia, 2. Specific classification principles for DM and IH.
(Coding Rules, March 2015)
Coding Rules - Current as at 16-Mar-2015 05:02 Page 13 of 28
Australian Consortium for Classification Development
Ref No: Q2890 | Published On: 15-Mar-2015 | Status: Current
ACCD Classification Information Portal
SUBJECT: Obstetric additional diagnosis sequencing
Q:
Is there a sequencing rule for the O80-O84 Delivery codes when they are assigned as an additional diagnosis? For example, if the principal diagnosis is an antepartum condition such as pre-eclampsia but the patient also has a perineal tear during the delivery, should the O80-O84 code immediately follow the antepartum principal diagnosis, that is, be sequenced as the second code?
A:
The Note at O80-O84 Delivery states:
‘Other abnormalities/complications classifiable elsewhere in Chapter 15 may be assigned in conjunction with codes O80-O84 to fully describe the delivery episode’.
There are no sequencing rules when codes from O84-84 Delivery are assigned as an additional diagnosis, apart from being sequenced before Z37.- Outcome of delivery, as in the instructional note at Z37.- :
‘Code first the delivery (O80- O84)’.
(Coding Rules, March 2015)
Coding Rules - Current as at 16-Mar-2015 05:02 Page 14 of 28
Australian Consortium for Classification Development
Ref No: Q2898 | Published On: 15-Mar-2015 | Status: Current
SUBJECT: Necrotising myopathy NOS
ACCD Classification Information Portal
Q:
How do you code necrotising myopathy? Is it necessary to assign R02 Gangrene, not elsewhere classified an additional code to specify the necrotising component?
A:
Assign G72.8 Other specified myopathies for necrotising myopathy NOS, by following the index pathway:
Myopathy G72.9
- specified NEC G72.8
The term ‘necrotising’ relates to muscle fibre necrosis, a feature of necrotising myopathy identified histologically in biopsied muscle tissue. Do not assign R02 Gangrene, not elsewhere classified to identify the necrosis.
(Coding Rules, March 2015)
Coding Rules - Current as at 16-Mar-2015 05:02 Page 15 of 28
Australian Consortium for Classification Development ACCD Classification Information Portal
Ref No: Q2904 | Published On: 15-Mar-2015 | Status: Superseded 15 December 2015
SUBJECT: Vacuum assisted wound closure (VAC) Dressings
Q:
Should VAC dressings be coded?
A:
Vacuum assisted wound closure (VAC) is a type of wound dressing which uses negative pressure to promote wound healing. The wound is covered with open cell foam or gauze dressing that moulds to the wound bed. A drainage tube is attached, the wound is then sealed and vacuum or negative pressure is applied via a pump. The suction pressure removes or ‘debrides’ loose tissue and has been shown to reduce swelling, aid wound closure and promote formulation of granulation tissue.
VAC dressings are classified in ACHI as a nonexcisional debridement and therefore assign the following code as appropriate when performed:
90686-01 [1628] Nonexcisional debridement of skin and subcutaneous tissue or
90686-00 [1627] Nonexcisional debridement of burn.
As VAC dressings are classified to nonexcisional debridement, ACS 0042 Procedures not normally coded, point 7 – Dressings, does not apply.
This will be clarified in ACS 0042 Procedures not normally code, point 7 – Dressings in a future edition.
(Coding Rules, March 2015)
Coding Rules - Current as at 16-Mar-2015 05:02 Page 16 of 28
Australian Consortium for Classification Development
Ref No: Q2906 | Published On: 15-Mar-2015 | Status: Current
ACCD Classification Information Portal
SUBJECT: Same-day chemotherapy for neoplasm; participant in clinical drug trial
Q:
A patient is admitted for same-day chemotherapy as part of a drug trial. What is the principal diagnosis?
A:
Where there is a clinical indication for same-day chemotherapy (for neoplasm), regardless of whether the chemotherapy was part of a drug trial, assign Z51.1 Pharmacotherapy session for neoplasm as principal diagnosis with an additional diagnosis code for the neoplasm.
Do not assign Z00.6 Examination for normal comparison and control for the above scenario. Z00.6 is located in category Z00 General examination and investigation of persons without complaint or reported diagnosis; codes from this category should not be assigned when there is a documented definitive diagnosis as the indication for chemotherapy.
Assign Z00.6 where the reason for admission is stated as being for a clinical trial for the purposes of research (without documentation of a clinical diagnosis).
Amendments to ACS 0026 will be considered for a future edition.
(Coding Rules, March 2015)
Coding Rules - Current as at 16-Mar-2015 05:02 Page 17 of 28
Australian Consortium for Classification Development
Ref No: Q2910 | Published On: 15-Mar-2015 | Status: Current
SUBJECT: O60 Preterm labour and delivery
ACCD Classification Information Portal
Q:
Does preterm labour and/or delivery have to meet the criteria in ACS 0002 Additional diagnoses before a code from O60 Preterm labour and delivery is assigned?
A:
The following are general guidelines for coding a delivery episode of care:
• follow the guidelines in ACS 0001 Principal diagnosis/Obstetrics to determine sequencing of codes for antepartum conditions and O80-O84 Delivery
• assign codes for conditions/complications (antepartum, labour and delivery, puerperal or non-obstetric) that meet the criteria in ACS 0002 Additional diagnoses and the guidelines in specific standards in Chapter
15 Pregnancy, childbirth and the puerperium of the ACS
• assign codes for the following (when applicable to the case):
O30 Multiple gestation
O60 Preterm labour and delivery
O09 Duration of pregnancy (see criteria in ICD-10-AM Tabular List)
• assign a code from Z37 Outcome of delivery
Codes from O60 Preterm labour and delivery must be assigned when onset of labour and/or delivery occurred before 37 completed weeks of gestation. Specific guidelines for assignment of O60 are included in
ACS 1511 Termination of pregnancy and 1550 Discharge/transfer in labour.
(Coding Rules, March 2015)
Coding Rules - Current as at 16-Mar-2015 05:02 Page 18 of 28
Australian Consortium for Classification Development
Ref No: Q2911 | Published On: 15-Mar-2015 | Status: Current
SUBJECT: Tongue channelling via coblation
ACCD Classification Information Portal
Q:
What is the correct procedure code for tongue channelling via coblation?
A:
The term ‘coblation’ means ‘controlled ablation’. Tongue channelling via coblation is also known as coblation tongue reduction, a technique that reduces the overall size of the tongue to eliminate snoring and sleep apnoea symptoms. The procedure is performed by applying radiofrequency energy to the base of the tongue through a probe, which is inserted into the deep tissue of the tongue. Radiofrequency energy causes shrinkage of the deep musculature and soft tissue of the tongue.
Where tongue channelling via coblation is documented, assign 45675-01[1665] Reduction of tongue size, by following the index pathway:
Reduction
- size
- - tongue (macroglossia) 45675-01 [ 1665 ]
Improvements to the ACHI Alphabetic Index will be considered for a future edition.
(Coding Rules, March 2015)
Coding Rules - Current as at 16-Mar-2015 05:02 Page 19 of 28
Australian Consortium for Classification Development
Ref No: Q2913 | Published On: 15-Mar-2015 | Status: Current
SUBJECT: Metallosis due to joint prostheses
ACCD Classification Information Portal
Q:
How do you code metallosis due to metal-on-metal joint prostheses (for example, total hip replacements)?
A:
Metallosis may occur due to the adverse effects of metal debris from metallic joint prostheses, particularly following total hip replacement.
The acetabular cup and implant head in metal-on-metal implants are composed of cobalt-chromium alloys.
Continuous movement of the hip joint results in micro-particles of metal being released into the soft tissues; these micro-particles may result in necrosis surrounding the implant or corrode and release metal ions into the systemic circulation resulting in elevated serum levels of chromium and cobalt. Metal poisoning occurs when toxic levels of these metals accumulate, leading to implant failure, tissue and bone necrosis, and organ damage.
Metallosis may result in localised or systemic effects, such as:
• tissue or bone necrosis or pseudotumour formation adjacent to the prosthesis
• cardiomyopathy or heart failure
• visual impairment, that may lead to blindness
• skin rashes
• nervous system dysfunction (cognitive impairment, memory loss, depression)
• thyroid dysfunction
Patients may describe joint pain, a metallic taste, headaches, anorexia and weight loss.
A revision procedure is required to replace the metal-on-metal implant with a nonmetallic implant (for example, ceramic and polyethylene).
As the metallosis is due to a breakdown of the prosthesis it is classified as a mechanical complication of the device. Therefore, where there is documented evidence of metallosis due to a joint prosthesis, assign:
T84.0 Mechanical complication of internal joint prosthesis
Y83.1 Surgical operation with implant of artificial internal device
Y92.22 Heath service area
Where documentation specifies that the patient has excessively high serum levels of cobalt or chromium, assign as an additional diagnosis:
R79.0 Abnormal level of blood mineral
As per the guidelines in ACS 1904 Procedural complications: An additional code from Chapters 1 to 19
should be assigned where it provides further specificity.
Additional codes for any specific manifestations should be assigned based on documentation in the clinical record and the criteria for code assignment in ACS 0002 Additional diagnoses.
(Coding Rules, March 2015)
Coding Rules - Current as at 16-Mar-2015 05:02 Page 20 of 28
Australian Consortium for Classification Development
Ref No: Q2918 | Published On: 15-Mar-2015 | Status: Current
ACCD Classification Information Portal
SUBJECT: External cause code for complication of vascular access device (portacath)
Q:
What external cause code is assigned with a complication code for vascular access device (eg portacath)?
A:
A vascular access device is an implanted venous catheter with a reservoir attached (see note in Z45.2
Adjustment and management of vascular access device).
When classifying a complication of a vascular access device (eg portacath), assign as the external cause of injury code:
Y83.1 Surgical operation with implantation of artificial internal device by following the index pathway Complication/implant, implantation/artificial/internal device.
(Coding Rules, March 2015)
Coding Rules - Current as at 16-Mar-2015 05:02 Page 21 of 28
Australian Consortium for Classification Development
Ref No: Q2920 | Published On: 15-Mar-2015 | Status: Current
SUBJECT: Urolift® procedure
ACCD Classification Information Portal
Q:
What is the correct code to assign for UroLift ® procedure?
A:
The UroLift ® procedure is a minimally invasive treatment for benign prostatic hypertrophy where small implants are permanently placed in the prostate through a cystoscope to hold back the enlarged prostate lobes in a retracted position so that it no longer blocks the urethra. Typically 4-6 implants are placed to retract the enlarged prostatic tissue. It is also known as prostatic urethral lift (PUL) procedure.
Assign:
90409-00 [1160] Implantation of other device(s), prostate, by following the index pathway:
Implant, implantation — see also Insertion
- device
- - prostate NEC 90409-00 [ 1160 ]
An additional code 36812-00 [1089] Cystoscopy should also be assigned as per ACS 0023
Laparoscopic/arthroscopic/endoscopic surgery.
Index amendments will be considered for a future edition of ACHI.
(Coding Rules, March 2015)
Coding Rules - Current as at 16-Mar-2015 05:02 Page 22 of 28
Australian Consortium for Classification Development
Ref No: Q2944 | Published On: 15-Mar-2015 | Status: Current
SUBJECT: Locked-in syndrome
ACCD Classification Information Portal
Q:
What code should be assigned for locked-in syndrome?
A:
Locked-in syndrome is a rare neuropsychological disorder. Its primary features are complete paralysis of voluntary muscles in all parts of the body except for those responsible for eye movements (Cardwell, 2013).
The most common aetiologies include haemorrhage or infarction of the basilar or vertebral arteries, brain injury, tumour or infection.
In 2013 WHO introduced a specific code for locked-in syndrome (G83.5) which has been incorporated into
ICD-10-AM Ninth Edition.
In the interim, assign G83.8 Other specified paralytic syndromes for this condition. Assign an additional code for the underlying cause of the paralytic syndrome, if known. For example, a patient was admitted with locked-in syndrome following a brain stem infarction, assign:
G83.8 Other specified paralytic syndromes
I63.9 Cerebral infarction, unspecified
See ACS 0001 Principal diagnosis, Problems and underlying conditions.
Reference:
Cardwell, M. S (2013). Locked-in syndrome. The Journal of Texas Medicine,109(2), e1.
(Coding Rules, March 2015)
Coding Rules - Current as at 16-Mar-2015 05:02 Page 23 of 28
Australian Consortium for Classification Development
Ref No: Q2945 | Published On: 15-Mar-2015 | Status: Current
ACCD Classification Information Portal
SUBJECT: Reversible cerebral vasoconstriction syndrome (RCVS)
Q:
How do you code reversible cerebral vasoconstriction syndrome (RCVS)?
A:
Reversible cerebral vasoconstriction syndrome is synonymously known as:
• acute benign cerebral angiopathy
• Call or Call-Fleming syndrome
• CNS pseudovasculitis
• isolated benign cerebral vasculitis
• reversible cerebral segmental vasoconstriction
• reversible cerebrovascular vasoconstriction syndrome
Reversible cerebral vasoconstriction syndrome is characterised by severe headaches, with or without other acute neurological symptoms, and diffuse segmental constriction of cerebral arteries that resolves spontaneously within 3 months.
There is currently no specific code or index pathway for reversible cerebral vasoconstriction syndrome in
ICD-10 (or ICD-10-AM). A submission will be sent to the WHO update reference committee (URC). In the interim, assign I67.8 Other specified cerebrovascular disease by following the index pathway:
Disease
- cerebrovascular
- - specified NEC I67.8
Enhancements to ICD-10-AM will be considered for a future edition.
(Coding Rules, March 2015)
Coding Rules - Current as at 16-Mar-2015 05:02 Page 24 of 28
Australian Consortium for Classification Development
Ref No: TN800 | Published On: 15-Mar-2015 | Status: Current
ACCD Classification Information Portal
Clinical update: Cystic fibrosis
Overview
Cystic fibrosis (CF) is a genetic disorder affecting mostly the lungs but also the pancreas, liver, kidneys and intestine. It can also be known as mucoviscidosis (“Cystic fibrosis”, 2015) and two thirds of patients are diagnosed by one year of age. CF is a disease with a wide diversity of clinical presentation, severity of symptoms, and rate of disease progression in the organs involved and the clinical manifestations will vary with the patient's age at presentation (Sharma, 2014).
Causes
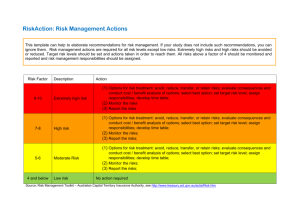
Cystic Fibrosis (CF) is a recessive genetic condition resulting from inheriting two copies of faulty gene from both parents (Cystic Fibrosis Australia, n.d.). The faulty gene is called the cystic fibrosis transmembrane conductance regulatory gene (known as the CFTR gene) and is responsible for creating a protein that moves salt and water out of a cell. If the CFTR gene is defective, this results in a build-up of thick, sticky mucus in the body's tubes and passageways. These blockages damage the lungs, digestive system and other organs, resulting in inflammation (swelling) and repeated infections (NHS Choices, 2014).In the lungs, the mucus clogs the tiny air passages and traps bacteria, resulting in repeated infections which can cause irreversible lung damage and death. In the pancreas, the thick mucus also stops digestive enzymes from reaching the small intestine, which leads to difficulty with digesting fats and absorbing some nutrients. This means that people with CF can have problems with nutrition (Better Health Channel 2012).
Figure 1: Cystic fibrosis – difference in the CFTR gene (University of Utah Health Sciences, n.d.)
Prevalence
• One in every 2,500 Australian babies, male or female, of Northern European ancestry.
• About one in 25 Australians of Northern European ancestry are carriers for the CFTR gene mutation.
• CF is less frequent in Southern European and Middle Eastern populations, and is rare or absent in Asian populations (Genetics in Family Medicine, 2007).
Complications
CF has a wide variety of complications across multiple body systems. These are related to the mucus deposits in various organs, leading to infections and difficulty with absorption of nutrients and vitamins.
Coding Rules - Current as at 16-Mar-2015 05:02 Page 25 of 28
Australian Consortium for Classification Development ACCD Classification Information Portal
Figure 2: What are the signs and symptoms of Cystic fibrosis? (National Heart, Lung, and Blood Institute, 2013)
Manifestations
The manifestations of CF affect multiple body systems including:
• respiratory
• gastrointestinal
• genitourinary
• endocrine.
Coding Rules - Current as at 16-Mar-2015 05:02 Page 26 of 28
Australian Consortium for Classification Development ACCD Classification Information Portal
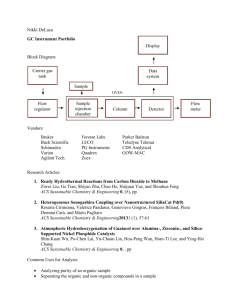
Figure 3: Manifestations of cystic fibrosis (Newson, 2012)
The image above identifies the potential manifestations of CF. Additional manifestations which may occur include:
• pulmonary hypertension
• fatty liver
• liver failure
• cholecystitis
• rickets (Sharma, 2014).
Management
CF has no cure, however, treatments have greatly improved in recent years. The goals of CF treatment include:
• preventing and controlling lung infections
• loosening and removing thick, sticky mucus from the lungs
• preventing or treating blockages in the intestines
• providing enough nutrition preventing dehydration (a lack of fluid in the body) (National Heart, Lung, and Blood Institute, 2013).
Treatment options include:
• antibiotics – to treat chest and lung infections
• intensive physiotherapy – to clear mucus from the lungs
• enzyme replacement capsules with food to aid digestion
• salt vitamin supplements
Coding Rules - Current as at 16-Mar-2015 05:02 Page 27 of 28
Australian Consortium for Classification Development ACCD Classification Information Portal
• bronchodilators – a type of medication that helps expand the airways inside the lungs, making it easier to breathe
• inhaled mucus-clearing treatments – such as Pulmozyme, hypertonic saline (a strong salt solution) and mannitol dry powder
• exercise – to help clear the airways and build core strength (Cystic Fibrosis Australia, n.d.; NHS Choices,
2014).
In some cases a lung transplant may eventually be required if the lungs become extensively damaged.
References:
Better Health Channel Victoria (2012). Cystic fibrosis. Retrieved from http://www.betterhealth.vic.gov.au/bhcv2/bhcarticles.nsf/pages/Cystic_fibrosisCystic Fibrosis Australia (n.d.). About Cystic Fibrosis. Retrieved from http://www.cysticfibrosis.org.au/all/about-cf/Genetics in Family Medicine: The Australian Handbook for General Practitioners (2007). Cystic
Fibrosis: Prevalence, Retrieved from https://www.nhmrc.gov.au/_files_nhmrc/file/your_health/egenetics/practioners/gems/sections/09_cystic_fibrosis.pdf Learn Genetics, Genetic
Science Learning Centre, University of Utah Health Sciences (2015). Cystic fibrosis: How do doctors diagnose cystic fibrosis? Retrieved from http://learn.genetics.utah.edu/content/disorders/singlegene/cf/National Heart, Lung, and Blood Institute (NIH), US department of Health Human
Services (2013). What are the signs and symptoms of cystic fibrosis? Retrieved from http://www.nhlbi.nih.gov/health/healthtopics/topics/cf/signsNational Heart, Lung, and Blood Institute (NIH), US department of Health Human Services (2013). How is cystic fibrosis treated? Retrieved from http://www.nhlbi.nih.gov/health/health-topics/topics/cf/treatment Newson, L. (2012). Cystic fibrosis: Presentation.
Retrieved from Patient.co.uk. Website: http://www.patient.co.uk/education/cystic-fibrosis Sharma, G.D. (2014). Cystic fibrosis clinical presentation.
Retrieved from: Medscape. Website: http://emedicine.medscape.com/article/1001602-clinicalNHS Choices (2014) Cystic fibrosis. Retrieved from http://www.nhs.uk/conditions/Cystic-fibrosis/Pages/Introduction.aspx
Coding Rules - Current as at 16-Mar-2015 05:02 Page 28 of 28