We thank the reviewers for their insightful comments, which have
advertisement

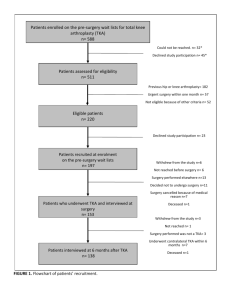
We thank the reviewers for their insightful comments, which have helped us improve the quality of this paper. Below are our point-by-point responses to the comments. Reviewer's report Title: Depression and Medical Comorbidity Predict Suboptimal Improvement in Knee Function after Total Knee Arthroplasty Version:3Date: 28 December 2013 Reviewer:Emérito-Carlos RODRIGUEZ-MERCHAN Reviewer's report: MAJOR COMPULSORY REVISIONS * The title should be changed: Depression in primary TKA and higher medical comorbidities in revision TKA seem to be associated with suboptimal subjective improvement in knee function Response: We have changed the title as suggested. The new title is as follows: “Depression in primary TKA and higher medical comorbidities in revision TKA are associated with suboptimal subjective improvement in knee function” * The way to define "depression" and "anxiety" is a great limitation of the article. Was the diagnosis confirmed by a phychologist or phychiatrist?. If the answer is yes, the paper is sound. If the answer is not, such a limitation makes the paper not sound (not acceptable). Response: Depression or anxiety was captured based on the presence of an ICD-9 code code for these conditions, which is usually captured in patient records based on a health care provider’s diagnosis. In most instances, this would be patients’ primary care provider or family practitioner, rather than a psychiatrist, since most depression is managed in the primary care setting in the U.S. We discussed this as a study limitation (see limitations section). We respectfully disagree that an absence of psychiatrist examination of a patient with depression, makes this study not worthy of publication. The use of ICD-9 diagnoses in epidemiological studies is not new, and has been done with its known limitations in both non-arthroplasty and arthroplasty literature. A psychiatrist diagnosis of depression is most ideal, but can’t be achieved in most epidemiological studies, given resource constraints and the practical challenges of examining every patient. In retrospective analyses of prospective data (as in our study) where psychiatrist referral for each patient had not been done for each patient with ICD-9 for depression years prior to the study, this is not possible. Even the well-funded cohort studies use validated questionnaires, due to issues with resources. A Pubmed literature search of “depression” and “arthroplasty” (with both in the title) done on 02/11/2014 found seven published studies, none of which used psychiatrist diagnosis of depression: ICD-9 codes were used in 3 studies [1-3]; three used depression scales [4-6]; and one used patient self-report [7]. Several studies published in non-arthroplasty literature have used non-psychiatrist examination methods for determining depression, e.g., validated depression questionnaires [8] or ICD-9 codes for depression [9], supporting the belief that studies with imperfect measures of depression can still contribute and help fill significant knowledge gaps. Again, we agree the best method in prospective studies would be examination, but this criticism may not be applicable to this retrospective cohort study. More importantly, the prevalence of depression using our ICD-9 codes was similar to that reported in studies of depression suing validated scales (see below). Several novel findings of our study make it worthy of publication and of interest to the readers. Our ability to include a large sample (5-10 times the highest sample in previous studies) as well as perform multivariable-adjusted analyses makes our findings robust and applicable, despite its limitations (which are listed in abstract, discussion and conclusions). “Since both anxiety and depression were captured based on presence of a diagnostic code, and psychological comorbidities may be under-recognized and under-diagnosed, it is likely that we missed some cases; however, the prevalence of depression is similar to the 9-15% reported in studies using validated instruments for depression [10-12]. This might have biased our estimates towards null, and we may have missed some important associations of anxiety and depression with outcomes. A retrospective study design did not allow us to have confirmation of depression/anxiety diagnosis by examination by a psychologist or a psychiatrist.” * In the text the Deyo-Charlson index includes 19 morbidities, but in table 1 only 6 of them have been included. It seems logical to include all of them in the table. Response: We have added all Deyo-Charlson index comorbidities in the table as suggested, see table 1. * In the ABSTRACT, in line 20 write depression and anxiety instead of physicological. In lines 21 and 23 write TKA instead of THA. In line 24 mention that there are 19 medical comorbidities. In line 25 mention that knee function means much better-better or same-worse. Also mention the great limitations of the study. Response: We have made all the recommended changes and regret the typographical errors. We have also added limitations to the abstract as suggested. “Conclusions: Depression in primary TKA and higher medical comorbidity in revision TKA cohorts were associated with suboptimal improvement in index knee function. Strategies focused at optimization of medical comorbidities, anxiety and depression pre- and perioperatively may help to improve TKA outcomes. Study limitations include the use of diagnostic codes, which may be associated with under-diagnosis of conditions and nonresponse bias.” * My recommendation is that the authors should divide their article in four clear parts (or articles): the relationship between depression and anxiety and subjective knee function after primary TKA; and after revision TKA; and the relationship between medical comorbidities and subjective knee after primary TKA; and after revision TKA. As I mentioned above, depression and anxiety should be better defined and diagnosed, Response: We have divided our result into four sections, as per reviewer recommendations. “Depression, anxiety and Improvement in Knee Function after Primary TKA At 2-years after primary TKA, 87% reported much better and 10% better knee function compared to preoperatively, and at 5-years, 85% and 10%, respectively. At 2-year follow-up, depression was associated with lower odds of much better knee function (p<0.01) in univariate analyses (Appendix 2) as well as lower odds of 0.5 of much better knee function (p=0.02) after multivariable-adjustment (Table 2). Anxiety was not associated with subjective knee function improvement at 2-years (p≥0.50). At 5-years, depression or anxiety were not significantly associated with knee function improvement (Table 2). Depression, anxiety and Improvement in Knee Function after Revision TKA At 2-years after revision TKA, 65% reported much better knee function and 20% better knee function compared to preoperatively, and at 5-years, 63% and 21%, respectively. In univariate analyses at 5-years after revision TKA, depression was associated with lower odds of much better knee function (p=0.05) (Appendix 3). In multivariable-adjusted analyses, this was no longer significant (p=0.17; Table 2). At 5years, in multivariable-adjusted analyses, neither depression nor anxiety were associated with knee function. Medical Comorbidity and Improvement in Knee Function after Primary TKA In univariate analyses, at 2-year follow-up, Deyo-Charlson index was associated with a statistically non-significant trend with much better knee function (p=0.10) (Appendix 2). This was no longer significant after multivariable-adjustment, (p=0.47) (Table 2). At 5-years, Deyo-Charlson index was not significantly associated with knee function improvement (p=0.25; Table 2). Medical Comorbidity and Improvement in Knee Function after Revision TKA In univariate analyses at 2 and 5-years after revision TKA, Deyo-Charlson had a non-statistically significant association with much better knee function (p=0.50 and 0.13; Appendix 3). In multivariable-adjusted analyses, higher Deyo-Charlson index was associated with significantly lower odds of 0.5 of much better knee function (p=0.05; Table 2) and a trend towards significantly lower odds of 0.4 of better knee function (p=0.07; Table 2) at 5-years. No significant associations were noted at 2-years (p>0.20). Level of interest: An article whose findings are important to those with closely related research interests Quality of written English: Acceptable Statistical review: No, the manuscript does not need to be seen by a statistician. Declaration of competing interests: I declare that I have not competing interest Reviewer's report Title:Depression and Medical Comorbidity Predict Suboptimal Improvement in Knee Function after Total Knee Arthroplasty Version:3Date: 1 February 2014 Reviewer:Shuji Taketomi Reviewer's report: The authors attempt to clarify whether medical and psychological comorbidity predicts patient satisfaction after TKA, by analyzing a large sample. Interestingly, depression in primary TKA and higher medical comorbidity in revision TKA cohorts were associated with poor improvement in patient satisfaction. Through the manuscript: “Knee function” after TKA usually means physical function such as walking, climbing, bathing and so on), however, it is used as subjective satisfaction in the manuscript. The use of the term “knee function” in this context may be misleading. Response: We have specified that this is subjective knee function assessment. Introduction Line 58: limitation(s) Response: We have made this correction as suggested. Methods Lines 89-99: Selection of outcome of interest seems to be an issue. The authors selected only “subjective” knee function evaluation as the outcome of interest. When discussing knee function following TKA, we usually use both objective outcome (range of motion, muscle strength, ###) and subjective outcome (KOOS, VAS, ###). The result that depression was associated with subjective outcome (patient satisfaction) may be a matter of course. Using not only subjective scale but also objective outcome scale may add value to this study. Response: We have specified that the function measure is subjective, by specifying this in the title, abstract and other parts of the paper. Line 112: [22][23,24] should be [22-24]. Response: We have made this change as recommended Results Lines 154-159: The authors state “patients were included in this study if they had ###completed the patient questionnaire”, however, they included all patients (7139 primary TKA###). It may be appropriate that the patient information of responders is included at Table1. Response: We clarified that we included patients who had responded to survey at either 2- or 5-years. Non-responder characteristics are provided in Appendix 1, which we have now presented as a table (table 2) according to the suggestion by the reviewer. We considered combining it with Table 1, however this would make table 1 uninterpretable and lead to 15 columns in the table and have several rows that are applicable only to survey responders. Line 156: “11” should be “Eleven”. Response: We have made this change as recommended Discussion Lines 191-193: I think this sentence is stated at inappropriate location. Response: We have made this change as recommended Lines 194-200: The authors explain the factors which contributed the result from only the point of view of rehab. In my opinion, subjective outcome of patients with depression naturally differs from that of mentally-normal patients. If this result mainly depends on rehabilitation, objective knee function should be different between the groups. Additionally, why was not depression associated with poor patient satisfaction at 5-years after TKA, vice versa at 2-years. Please discuss from these point. Response: We agree and have added this to the discussion as recommended “An interesting finding from our study was the association of depression with suboptimal improvement in index knee function 2-years after primary TKA. Several factors may contribute. Depressed patients are less likely to successfully complete rehabilitation therapy [13, 14] that is required post-TKA. They may not follow-up with their surgeon regularly due to concomitant depression and may have worse post-operative pain, which may impact adherence with rehabilitation therapy. Optimal physical rehabilitation after TKA is the key to best results after TKA [15, 16]. The absence of this association at 5years may be either due to a smaller sample size making it underpowered analysis or due to “catching up” by patients with depression after 2-years. Lines 221-222: If it is correct, why did the study of primary TKA result in a different outcome from that of revision TKA? Response: We discuss this in the discussion section. “An interesting finding from our study was the association of depression with suboptimal improvement in index knee function 2-years after primary TKA. Several factors may contribute. Depressed patients are less likely to successfully complete rehabilitation therapy [13, 14] that is required post-TKA. They may not follow-up with their surgeon regularly due to concomitant depression and may have worse post-operative pain, which may impact adherence with rehabilitation therapy. Optimal physical rehabilitation after TKA is the key to best results after TKA [15, 16]. The absence of this association in primary TKA at 5-years may be either due to a smaller sample size making it underpowered analysis or due to “catching up” by patients with depression after 2-years. The differences in findings between primary and revision TKA may be due to differences in patient characteristics (depression, mean Deyo-Charlson index), the underlying diagnosis and in the rate of complications between primary and revision TKA.” Abstract Line 21: “Total hip arthroplasty (THA)” should be “total knee arthroplasty (TKA)”. Line 23: “THA” should be “TKA”. Line 26: Again, “THA” should be “TKA”. Response: We regret these errors and have corrected them as recommended. Lines 28-29: Comment is same for lines 154-159. Please see above. Lines 35-38: These statements do not match with those of the conclusions section in the context (Lines 251-254). I feel the contents in the context better reflect the study results. Response: We have modified and corrected these conclusions in the abstract. “Conclusions: Depression in primary TKA and higher medical comorbidity in revision TKA cohorts were associated with suboptimal improvement in index knee function. It remains to be seen whether strategies focused at optimization of medical comorbidities and depression pre- and peri-operatively may help to improve TKA outcomes. Study limitations include the use of diagnostic codes, which may be associated with under-diagnosis of conditions and non-response bias.” Keywords “Total knee arthroplasty” may be more appropriate than “total knee replacement”. Response: We agree and have corrected this. Level of interest:An article whose findings are important to those with closely related research interests Quality of written English:Acceptable Statistical review:Yes, but I do not feel adequately qualified to assess the statistics. Declaration of competing interests: I declare that I have no competing interests. References: 1. Browne JA, Sandberg BF, D'Apuzzo MR, Novicoff WM: Depression Is Associated With Early Postoperative Outcomes Following Total Joint Arthroplasty: A Nationwide Database Study. J Arthroplasty 2013. 2. Stundner O, Kirksey M, Chiu YL, Mazumdar M, Poultsides L, Gerner P, Memtsoudis SG: Demographics and perioperative outcome in patients with depression and anxiety undergoing total joint arthroplasty: a population-based study. Psychosomatics 2013, 54(2):149-157. 3. Singh JA, Lewallen D: Age, gender, obesity, and depression are associated with patientrelated pain and function outcome after revision total hip arthroplasty. Clin Rheumatol 2009, 28(12):1419-1430. 4. Perez-Prieto D, Gil-Gonzalez S, Pelfort X, Leal-Blanquet J, Puig-Verdie L, Hinarejos P: Influence of depression on total knee arthroplasty outcomes. J Arthroplasty 2014, 29(1):44-47. 5. Nickinson RS, Board TN, Kay PR: Post-operative anxiety and depression levels in orthopaedic surgery: a study of 56 patients undergoing hip or knee arthroplasty. J Eval Clin Pract 2009, 15(2):307-310. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. Brull R, McCartney CJ, Chan VW: Do preoperative anxiety and depression affect quality of recovery and length of stay after hip or knee arthroplasty? Can J Anaesth 2002, 49(1):109. Riddle DL, Wade JB, Jiranek WA: Major depression, generalized anxiety disorder, and panic disorder in patients scheduled for knee arthroplasty. J Arthroplasty 2010, 25(4):581-588. Ruo B, Rumsfeld JS, Hlatky MA, Liu H, Browner WS, Whooley MA: Depressive symptoms and health-related quality of life: the Heart and Soul Study. JAMA 2003, 290(2):215-221. Melfi CA, Chawla AJ, Croghan TW, Hanna MP, Kennedy S, Sredl K: The effects of adherence to antidepressant treatment guidelines on relapse and recurrence of depression. Archives of general psychiatry 1998, 55(12):1128-1132. Ma Y, Balasubramanian R, Pagoto SL, Schneider KL, Hebert JR, Phillips LS, Goveas JS, Culver AL, Olendzki BC, Beck J et al: Relations of Depressive Symptoms and Antidepressant Use to Body Mass Index and Selected Biomarkers for Diabetes and Cardiovascular Disease. Am J Public Health 2013, 103(8):e34-e43. Zhang X, Bullard KM, Cotch MF, Wilson MR, Rovner BW, McGwin G, Jr., Owsley C, Barker L, Crews JE, Saaddine JB: Association between depression and functional vision loss in persons 20 years of age or older in the United States, NHANES 2005-2008. JAMA ophthalmology 2013, 131(5):573-581. Li C, Ford ES, Zhao G, Tsai J, Balluz LS: A comparison of depression prevalence estimates measured by the Patient Health Questionnaire with two administration modes: computer-assisted telephone interviewing versus computer-assisted personal interviewing. International journal of public health 2012, 57(1):225-233. McGrady A, McGinnis R, Badenhop D, Bentle M, Rajput M: Effects of depression and anxiety on adherence to cardiac rehabilitation. Journal of cardiopulmonary rehabilitation and prevention 2009, 29(6):358-364. Glazer KM, Emery CF, Frid DJ, Banyasz RE: Psychological predictors of adherence and outcomes among patients in cardiac rehabilitation. Journal of cardiopulmonary rehabilitation 2002, 22(1):40-46. Brueilly KE, Pabian P, Straut L, Freve L, Kolber M: Factors contributing to rehabilitation outcomes following hip arthroplasty. Physical Therapy Reviews 2012, 17(5):301-310. Bade MJ, Stevens-Lapsley JE: Early high-intensity rehabilitation following total knee arthroplasty improves outcomes. J Orthop Sports Phys Ther 2011, 41(12):932-941.