Human and Non Human Primate product form
advertisement

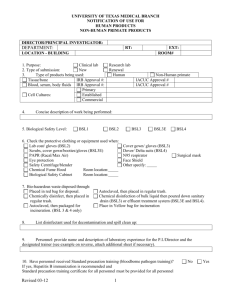
UNIVERSITY OF TEXAS MEDICAL BRANCH NOTIFICATION OF USE HUMAN AND NON HUMAN PRIMATE PRODUCTS PRINCIPAL INVESTIGATOR: DEPARTMENT: OFFICE BUILDING/ROOM NUMBER: LAB BUILDING/ROOM NUMBER: ROUTE: 1. Purpose: Clinical Lab 2. Type of submission: New 3. Type of products used: Human Tissue, bone IRB Approval #: Blood, serum, body fluids IRB Approval #: Primary: Cell Cultures Established: Commercial: EXT: Research Lab Renewal Amendment (NOU #: Non Human Primate IACUC Approval #: IACUC Approval #: ) 4. Concise description of work performed (include specific techniques used): 5. Biological Safety Level: BSL2 BSL3 BSL3E BSL4 6. In addition to eye protection, check the personal protective equipment (PPE) worn when handling agent(s) in vitro: Lab coat/gloves/eye protection (BSL2) Cover gown/gloves/eye protection (BSL3) Scrubs/cover gown/ gloves (BSL3E) Positive pressure suits (BSL4) Face Shield Other specify: Surgical mask N95 respirator Full/half-face respirator PAPR 7. Check lab equipment used when handling agent(s) in vitro: Centrifuge, type: Blender Homogenizer, type: Sonicator Shaker Chemical Fume Hood: Biological Safety Cabinet: Other specify: Building/Room: Building/Room: Building/Room: Building/Room: 8. Method for disposal of biohazardous waste: Placed in red bag for disposal. Autoclaved, then placed in regular trash. Chemically disinfected, then placed in regular trash. Placed in yellow bag for incineration. Chemical disinfection or autoclave of bulk liquid, then poured down sanitary drain or BSL3E/BSL4 effluent treatment system. Autoclaved, then packaged for incineration. Other: Revised: 10/20/2015 9. List disinfectant(s) used for surface decontamination and spills: Cavicide MicroChem % Bleach % Other % 10. Complete the personnel experience table at the following link: Personnel Experience Table Attached 11. Have personnel completed the online Standard Precautions training? Yes No Please attach Standard Precautions certificates for all personnel. Online Bloodborne pathogen training is required to be completed every two years for non-select agent users and every year for select agent users. __________________________________________ PI Signature Date Institutional Biosafety Committee Use Only _______________ Date Approved _______________ Date for Resubmission ___________________________________ Chairman Signature Revised: 10/20/2015 ________________ NOU Number ______________________________________ Print Name