Foot Ulcer Healing in Patients with Diabetes and Chronic Kidney
advertisement

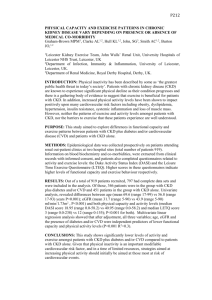
P91 FOOT ULCER HEALING IN PATIENTS WITH DIABETES AND CHRONIC KIDNEY DISEASE (CKD) Hicks, L, Kumwenda, M, Wordsworth, S, Somalanka, S, Swidan, A Renal and Diabetes Unit, Glan Clwyd Hospital BACKGROUND: Chronic Kidney Disease (CKD) and Diabetes are an unfortunate combination of diseases which may lead to limb threatening complications. The combination of vascular changes and peripheral neuropathy put the foot at risk and development of complex foot ulcers is not unusual. There is a large amount of data available for diabetic foot disease and its management; however there is substantially less available relating to patients who have both these diseases. It was decided to review management and outcomes for this patient group, to establish a baseline to guide potential changes in practice. DESIGN METHOD: Patients who were known to both the CKD clinic and the Multidisciplinary diabetic foot clinic (MDFC) over a period of 3 years were identified, 55 patients were found, 41 male. A retrospective audit of their management and outcomes was completed. It included gender, type and duration of diabetes; stage of CKD; Cardiovascular risk factors; Existing complications; Foot risk factors; Biochemistry; Microbiology of the ulcer; Drug management of risk factors and outcomes for healing. The annual number of MDFC attendees was 260. RESULTS: Mean age male58 (range37-85), female65 (range52-87). Incidence of risk factors, diabetes type, CKD stage, complications and ulcer outcomes were noted (Table1&2). Table1: Numbers with Risk Factors/ complications BMI >30 25 Previous CVA 9 Smokers 8 Absent protective sensation 41 Previous MI 14 Retinopathy 30 dislipidaemia 47 Peripheral Arterial Disease (PAD) 27 hypertension 51 ED 12 Type1 diabetes mellitus 14(2 female) CKD stage 3 27 Type2 diabetes mellitus 41(12female) CKD stage 4 9 CKD stage 1&2 11 CKD stage 5 haemodialysis 8 13 patients had angiograms of which 9 were amenable to angioplasty. Table2: Ulcer outcomes during the study period Healed Partially healed worse Amputation Ulcer 37 11 6 7 osteomyelitis 1 0 0 0 4 cases were referred to DFC with ulcers - later proven not to have diabetes, all healed; mean healing time 4.2months (range2-6). Average healing time for the study group as a whole was 9 months (range1-36) compared with average healing time of 2 months for all the MDFC attendees during a year. Patients who presented late with ulceration had poorer outcomes.5 patients had amputation associated with a none healing ulcer; 24 amputations occurred in all MDFC attendees without CKD over the same period. 11 died during the study period, only 2 of these had a healed ulcer, 4 had well controlled diabetes, 1 was on dialysis. CONCLUSION: This review suggests that patients who suffer from CKD and diabetes have more comorbidities/complications, take longer to heal and are less likely to heal than patients with foot ulcers and just diabetes or just CKD. There is currently a well-publicised drive to improve outcomes for people with diabetes; however there are particular difficulties in addressing the needs of CKD patients with diabetes. Prevention of ulcerations in the first place would seem to be ideal. 50% of hospital acquired foot pressure sores occur in patients with diabetes; it’s not clear what proportion have CKD. Introduction of education, for ward staff in general as well as CKD patients and their carers, on the prevention of foot ulceration would seem a logical step. Early referral of ulceration to the MDT DFC would offer best opportunity to achieve healing.