workshop_datainterpretation - OSCE-Aid
advertisement

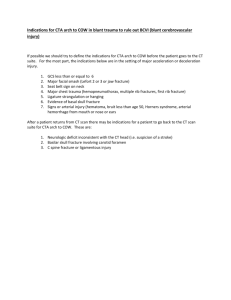
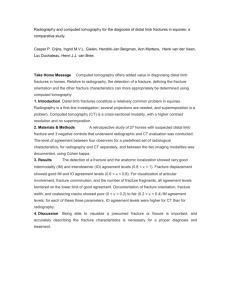
OSCE-Aid Revision Workshops: Data interpretation Data Interpretation: additional resources This resource covers interpretation of Abdominal Radiographs, Orthopaedic Radiographs and Blood Test Resutls. Please see the other listed documents on the data interpretation page to cover: Chest Radiographs, Urine Dipstick Analysis, Spirometry, and Arterial Blood Gases. Section1: Interpreting Abdominal Radiographs Systematic approach: 1. Demographics and details: ‘This is an abdominal radiograph taken of … on … at …. 2. View- type and adequacy: ‘It is a supine AP view and of adequate view as I can visualize the hemidiaphragms to the hernial orifices’ a. Supine AP view is standard. Decubitus view would be when lying on their side. b. Usually require 2 views to get adequate visualization from diaphragms to hernial orifices. If this area isn’t adequately visualized then can comment on needing another view. 3. Penetration 4. Bowel gas pattern: a. Stomach b. Small bowel- valvulae coniventes (centrally positioned, span whole diameter of the bowel’) c. Large bowel- haustra not going all the way across the diameter of the bowel, usually have a mottled appearance as contain air, positioning is fixedascending, descending colon and rectum are usually clear to identify. 5. Soft tissues (trace around and comment on): a. Lung bases b. Liver and spleen c. Psoas (iliacus and psoas muscles form the iliopsoas muscle attached to the greater trochanter of the hip- they are the hip flexors.) d. Kidneys- trace down ureters to bladder 6. Bones a. Ribs b. Vertebrae c. Pelvis d. Femurs 7. Additional calcifications and artefacts a. Eg gallstones, mesenteric LN calcification, costochondral calcification, phleboliths, fibroids 8. Summary: a. ‘In summary this is an a supine AP abdominal radiograph taken of … on … with the main positive finding being …. This could be consistent with a diagnosis of …’ Examples of main findings Abnormal bowel gas patterns: - Pneumoperitoneum- air under the diaphragm or free gas can sometimes be seen between the loops of bowel. **In an acute abdomen should always request an erect chest X-ray. - Rigler’s sign- the bowel appears double walled as there is air either side of the bowel © 2016 www.osce-aid.co.uk OSCE-Aid Revision Workshops: Data interpretation - - - - - Football sign: air risen to the front of the diaphragm creating a football appearance Small bowel obstruction: >5cm distended small bowel. Centrally located, valvulae coniventes (spanning the whole diameter of the small bowel). Commonest causes: adhesions, Crohn’s, tumours, hernias. Large bowel obstruction: >6cm colon, >9cm caecum. Peripherally located, haustra (not spanning full diameter of bowel). Commonest causes: CRC, diverticular disease, hernias, volvulus, pseudoobstruction (no mechanical cause but presents the same, mostly in the elderly) Volvulus- commonest types o Sigmoid volvulus: sigmoid twists at it’s own mesentry in LIF. Coffee bean sign pointing towards diaphragm. o Caecum volvulus: 20% have a congenital malformation that means can twist on it’s own mesentry. Thumb-printing: mucosal thickening of haustral heads and increased space between bowel= inflammatory bowel disease. (Colitis of any cause, most common of which is IBD). Lead pipe colon: loss of normal haustra in transverse colon= longstanding UC Toxic megacolon: dilatation of bowel in absence of obstruction and presence of acute bowel disease. Causes: IBD esp UC, colitis of other cause eg infection ***Please see radiologymasterclass.com for great examples of these radiographs*** © 2016 www.osce-aid.co.uk OSCE-Aid Revision Workshops: Data interpretation Practice question: A 27 year old woman presents to A&E with vomiting and abdominal pain. She previously had surgery for bowel obstruction. The below AXR is taken. Please practice present the XR and give a differential for your findings. Name: Mallory Weiss, DOB 1/1/1980, HN 5768958 Date of study: 12/1/2016, time 11:06am Image from radiologymasterclass.com © 2016 www.osce-aid.co.uk OSCE-Aid Revision Workshops: Data interpretation Model answer - This is a supine AP abdominal XR taken of MW DOB 1/1/1980 HN 5768958, on the 12/1/2016 at 11.06. - It displays a view from the lower thoracic cavity to the ischial spines of the pelvis. This is an inadequate view as I would like to visualize the hemidiaphragms to the hernial orifices. - Examining the bowel first I can see a central area of distended bowel with the appearance of valvulae coniventes. This is likely to be small bowel. I cannot visualize the stomach or the large bowel. - Examining the area of the liver, spleen, kidneys, and psoas muscles there are no abnormalities displayed. - There appears to be no bony injuries of the visible ribs, vertebrae or pelvic crests. - There are no abnormal calcifications, however in the right upper quadrant there appears to be evidence of previous surgery. There are no additional artefacts. - In summary this is a supine AP abdominal XR taken of .. on ... with the main positive findings being that there appears to be small bowel distension caused by small bowel obstruction. There is evidence of previous abdominal surgery which could indicate an anastamosis. In this context and a history of previous bowel obstruciton, a likely cause could be adhesions causing obstruction. Additional differentials would include Crohn’s disease, hernias and tumours. Abnormal soft tissues and bones: - Organomegaly- spleen and liver - Hydronephroiss - Masses - Fractures and OA - Bone mets - Paget’s disease- expansion and coarsening of trabecular pattern Abnormal calcifications: - renal calcification - nephrocalcinosis - ureteric calcification - bladder stones (urinary stasis) - vascular calcification - AAA- if wall calcified - Chronic pancreatitis with calcification - Adrenal gland calcification - Gallstones and mesenteric LN calcification Artefacts - IVC filters - Pigtail/JJ stents - Foreign bodies © 2016 www.osce-aid.co.uk OSCE-Aid Revision Workshops: Data interpretation Section 2: Interpreting Orthopaedic Radiographs Systematic approach: 1. Demographics ‘this is a radiograph taken of … on … at …’ 2. Film details: a. AP/lateral and comment on whether additional view is needed b. Penetration c. Adequate view of what bone is being shown 3. What is shown anatomically in the radiograph 4. Describe the fracture seen: a. Where: where fracture is- if in long bones split bone into 3rds for description, use anatomical landmarks where possible b. Type: there is a spiral/transverse/oblique fracture c. Displaced/undisplaced/minimally displaced d. Rotation/translocation/angulation/shortening/shift (ensuring you are describing the distal portion in relation to the proximal portion) e. Additional features you must comment on if present: i. Comminuted/wedge shaped ii. Avulsion fracture (portion of bone pulled away by ligament/tendon). iii. Stress fracture (repeated low impact trauma to bone- will see periosteal reaction in subtle calcification of bone but no clear fracture). iv. Dislocation and subluxation v. Diastasis (separation of 2 bones that are usually adjacent eg of pubic symphysis- orthopaedic emergency) 5. Additional factors: soft tissue swelling, foreign bodies. 6. Summary: a. This is a AP/lateral view of the L knee taken of … on the … at … The main positive findings are (describe fracture seen succinctly) b. This is in keeping with… (classification system if relevant for fracture shown) c. The management of this fracture would include i. DR ABCDE ii. Full history paying particular attention to the mechanism of injury and examining the injury. iii. Treatment would include: 1. ANALGESIA!!!! 2. Conservative management: sling/POP/traction and follow up in fracture clinic OR 3. Surgical management if open/ unstable/ complex/ polytrauma/ pathological/ nerve or BV involvement. Can be internal fixation (IM nails and plates) or external fixation. Orthopaedic follow up. d. If relevant- say you would like to compare against old radiographs Important discussion points that are easy to ask you about! Principles of wound management (RIR) - REDUCE - IMMOBILISE - REHABILITATION Open wound management 1. DR ABCDE 2. History and examination 3. Tetanus booster 4. Clean and inspect the wound 5. Lavage, debride, remove necrotic tissue © 2016 www.osce-aid.co.uk OSCE-Aid Revision Workshops: Data interpretation 6. Surgery 7. Antibiotics e.g. cefuroxime and metronidazole Complications of fractures Early complications Wound infection Fat embolism Compartment syndrome ARDS Chest infection DIC Exacerbate general illness Late complications Deformity OA Aseptic necrosis Reflex sympathetic dystrophy © 2016 www.osce-aid.co.uk OSCE-Aid Revision Workshops: Data interpretation Practice question 1: Dorothy Branning, DOB 3/1/1930, HN 3647598 Date of study: 5/1/2016, time 14:30. L wrist. Image from radiologymasterclass.com 1. Please present your findings. 2. What would your management be? © 2016 www.osce-aid.co.uk OSCE-Aid Revision Workshops: Data interpretation Model answer - Displayed are radiographs taken of DB DOB HN at 14:30 on 5/1/2016. The radiographs show an AP and a lateral view of the left wrist displaying a view from the metacarpals, carpal bones and distal half of the forearm. - There is adequate penetration and an adequate view of the wrist. - There is a transverse fracture that can be seen at the distal radius above the level of the radioulnar joint with dorsal angulation and displacement of the hand. There is notably no ulnar fracture. I cannot see any other bony injuries. - There is soft tissue swelling surrounding the wrist, most notably on the ventral side. - There are no other findings. - In summary this is a lateral and an AP radiograph taken of the left wrist of … on … at… Main positive findings are a transverse fracture of the distal radius above the level of the radioulnar joint and no associated ulnar styloid fractures. This is therefore a frykman type 1 fracture. There is dorsal displacement of the hand and surrounding soft tissue swelling. - This is consistent with a colles fracture. - Management of this fracture would include o A thorough DR ABCDE assessment o Taking a full history paying particular attention to the mechanism of injury and full examination looking for any other injuries o The patient will require analgesia and then will likely be managed conservatively although I would like orthopaedic input. o Treatment of the fracture would include Reduction, immobilization and rehabilitation Following reduction, immobilization would likely be carried out with POP cast and then follow up in fracture clinic. Further investigation into bone density would be important in the OP setting. © 2016 www.osce-aid.co.uk OSCE-Aid Revision Workshops: Data interpretation Practice question 2: Name: Jeremy Hubbard, DOB 8/10/1960 HN 8907327 Study date: 5/1/2016, time 11:06am Image from radiologymasterclass.com 1. Please present your findings. 2. How would you manage this patient? © 2016 www.osce-aid.co.uk OSCE-Aid Revision Workshops: Data interpretation Model answer - These radiographs display an AP and lateral view of the R ankle of JH DOB HN. They are taken on the … at … - The radiographs show views of the distal third of the lower tibia and fibula to the proximal metatarsal bones. This is an inadequate view as I would also like to visualize the proximal tibia and fibula. - There film is of adequate quality. - There are a number of fractures visible, I will describe each in turn: o There is a transverse fracture of the medial malleolus which appears minimally displaced inferiorly. o There appears to be a fracture of the distal tibia which on lateral view can be determined to be a posterior malleolus fracture that is posteriorly displaced. o There is also a spiral fracture of the fibula above the level of the tibio-fibular syndesmosis. o The talus is displaced posteriorly and laterally in addition to the lateral and medial malleolus bone fragments. o The joint space is widened anteriorly and at the tibio-fibular syndesmosis with lateral talar shift which indicates that the joint in unstable. - As mentioned I would like to visualize the proximal fibula to determine whether there could be a Maisonneuve fracture. - In summary, these are AP and lateral radiographs showing the R ankle of JH taken on… There are 3 visible fractures involving both medial and lateral malleoli, with talar shift and unequal joint space resulting in an unstable joint. I would like an additional proximal view including the proximal fibula. Management of this fracture would include: o DR ABCDE o Full history and examination paying particular attention to the neurovascular status of the foot. o Analgesia o Orthopaedic input as this is a complex fracture picture and is likely to require surgery for definitive treatment. This could consist of internal or external fixation. © 2016 www.osce-aid.co.uk OSCE-Aid Revision Workshops: Data interpretation Additional revision points and important classifaction systems to be aware of: - Hip fractures (know how to describe them well!) with GARDEN CLASSIFICATION o Type 1- incomplete or impacted bone injury with valgus angulation of the distal component o Type 2- complete fracture (across whole neck), undisplaced o Type 3- complete fracture, minimally displaced o Type 4- complete fracture, totally displaced - ALLMAN CLASSIFCATION: Clavicular fractures o Type 1- middle 3rd o Type 2- distal 3rd o Type 3- proximal 3rd - FRYKMAN CLASSIFICATION: Wrist fractures http://jbjs.org/content/80/4/582 - WEBER CLASSIFICATION: Ankle fractures o Weber A- fracture of lateral malleolus, below level of syndesmosis o Weber B- fracture of lateral malleolus, usually below the syndesmosis but extending more proximally then type A. Medial malleolus may be fractured. o Weber C- fracture of lateral and medial malleolus. Fracture above level of syndesmosis. Unstable. © 2016 www.osce-aid.co.uk OSCE-Aid Revision Workshops: Data interpretation Case courtesy of A.Prof Frank Gaillard, Radiopaedia.org, rID: 9642 © 2016 www.osce-aid.co.uk OSCE-Aid Revision Workshops: Data interpretation Section 3: Interpreting Blood Results Bloods results that are most likely to come up and you should know well include: - Liver function tests - Thyroid function tests - Haematinics - Electrolyte derangement For each you should be able to interpret common pictures and list main differentials and treatment options. Here we will cover electrolyte derangement as this is often most confusing or not covered well in teaching. Practice question: Mrs Kleiner, a 72 year old lady, has attended GP feeling increasingly tired. She has a history of congestive cardiac failure, hypertension and chronic kidney disease. She is on a number of medications shown below. She has attended to discuss blood test results taken on her last visit. Please review her results and discuss them with her, formulating a management plan. Medication list Losartan Ramipril Furosemide Spironolactone Oxybutynin Salbutamol Budesonide U&Es K 5.4 (3.5-5 mmol/L) Na 149 (135 -145mmol/L) Ur 14 (2.5-7.8mmol/L) Cr 130 (68-118mmol/L) © 2016 www.osce-aid.co.uk OSCE-Aid Revision Workshops: Data interpretation Model answer These questions usually come in the setting of a communication station and may incorporate multiple skills- consultation skills, explaining skills, checking understanding and management formation skills. Always look carefully at the medication list!! - - - - - - Introduction and setting scene o Introduce, explain and consent patient for discussion o Check understanding of why test has been done and what is causing her symptoms. Does she have any concerns? o How has she been since last visit/bloods taken o Explain took a routine blood test to determine the level of salts in the body which can be altered by many things including medications, how kidneys functioning etc. A few of these have come back slightly abnormal which could be caused by lots of things. For that reason would like to ask a few questions and see if we can find out why and then possibly make a few changes to rectify the blood tests, is that ok? History- check for signs of hyperkalaemia- keep it brief and concise o Symptoms: chest pains/palpitations/problems with water works/ feeling sick/ abdominal pain or constipation/weakness. o Cause: can see on spironolactone and ramipril- how long have you been on these? Any new medications? Any known kidney problems? Any other medical conditions (DM/addison’s/kidney disease). Explaining o The tests that we’ve done show that the level of potassium in the blood is slightly higher than normal. This could be because of a few factors, most likely being that 2 of your medications, ramipril and spironolactone can increase the level of K in the blood. o The other factor is that with your kidney disease, sometimes you can get a rise in K as it’s not being excreted from the body so effectively. Form a management plan o For that reason along with the fact that you don’t have any symptoms and you’re well, I would like to do a few things today. Firstly I would like to get an ECG. If everything is ok with that then I would want to stop the spironolactone and then get you back in 5-7 days for a repeat blood test which will tell us if we’ve done enough to treat it. o Chunk and check as you go along Safety net o In the meantime if you feel…. All symptoms… then please come straight back or attend A&E. Check understanding and answer any questions Close © 2016 www.osce-aid.co.uk OSCE-Aid Revision Workshops: Data interpretation POTASSIUM Hypokalaemia ECG changes 1. U waves 2. Tall tented P waves 3. Increased PR interval Hyperkalaemia ECG changes 1. Tall tented T waves 2. Sine wave appearance 3. Absent/small P waves 4. Broad QRS 5. VF Presents - Muscle cramps and weakness - Lethargy - Palpitations Presents - Arrhythmias - Palpitations - Chest pain - Constipation - Weakness Causes: 1. DRUGS a. Insulin b. Salbutamol c. Loops and thiazide diuretics d. Laxatives e. Steroids 2. Endocrine a. Cushing’s b. Conn’s 3. GI a. Diarrhoea and vomiting b. Villous adenoma- profuse diarrhoea 4. Renal a. Gitelman’s syndrome b. Barterr’s syndrome c. Liddle’s syndrome Causes 1. DRUGS a. Spironolactone b. ACEi c. Suxamethonium d. Blood transfusion e. Excessive K replacement 2. Endocrine a. Addison’s disease b. DM with metabolic acidosis 3. Renal a. Rhabdomyolysis b. RTA4 4. Other a. Burns Management- dependent on severity 1. >2.5 PO replacement 2. <2.5 IV replacement e.g: 40 mmol potassium in 1L 0.9% saline over 8 hours. Management- dependent on severity 1. Stabalise myocardium: 10ml of 10% calcium gluconate 2. Drive K into the cells: 10 units short acting insulin in 50ml 50% dextrose, 5mg salbutamol (nebulized) 3. Sodium bicarbonate- according to venous bicarbonate eg 500mg 4. Careful fluid resuscitation © 2016 www.osce-aid.co.uk OSCE-Aid Revision Workshops: Data interpretation SODIUM Hyponatraemia Presents - Nausea and malaise - Headache - Irritability - Confusion - Weakness - Reduced GCS and seizures - Coma and death Causes: 1. Hypervolemic (oedemtous) a. Nephrotic syndrome b. Cardiac failure c. Liver cirrhosis d. Renal failure 2. Euvolemic determine if urine osmolality >100mmol/kg a. >100= SIADH b. <100= water overload, severe hypothyroidism, glucocorticoid insufficiency 3. Hypovolemic (dehydrated) determine whether urinary Na >20mmol/L a. >20= addison’s, renal failure, diuretic excess, osmolar diuresis (increased glucose/urea) b. <20= diarrhoea, vomiting, fistulae, small bowel obstruction, CF Management 1. OVERALL!!! Involve seniors, endocrine team and ITU early on. 2. Dependent on cause: a. Hypovolemia: 0.9% saline slowly. Check U&Es BD and aim not to exceed increasing Na by >10mmol in 24 hours b. Hypervolemia eg CCF: fluid restrict and give furosemide c. Euvolemic eg SIADH: fluid restrict and consider further drugs. 3. RISK: central pontine myelinosis if too quick! Hypernatraemia Presents - Lethargy - Thirst - Weakness - Irritability - Confusion - Seizures - Coma and death Causes 1. Diarrhoea, vomiting, burns 2. DI 3. Diabetic coma 4. Iatrogenic- excessive saline Management 1. PO water 2. 5% dextrose IV slowly (if hypovolemic can give 0.9% saline) 3. (Risks fluid shift in brain if changed too quickly) © 2016 www.osce-aid.co.uk OSCE-Aid Revision Workshops: Data interpretation CALCIUM Hypocalcaemia ECG changes 1. Prolonged QT interval Hypercalcaemia Presents: SPASMODIC - Spasms- Trousseau’s sign - Perioral parasthesia - Anxious, irritable, irrational - Seizures - Muscle tone increased- smooth muscle eg wheeze - Orientation impairment - Dermatitis - Impetigo herpetiformis - Chvostek’s sign/ cataracts/ CM/ choreoathetosis Presents: bones, stones, moans, groans - Bone pain and fractures - Renal stones - Polydipsia - Polyuria - Depression and irritability - Abdominal pain - Contipation - Spasms Causes: 1. DRUGS a. Furosemide 2. Hypoparathyroidism 3. Pseudohypoparathyroidism 4. Vitamin D deficiency 5. Acute pancreatitis 6. Acute rhabdomyolysis Causes 1. DRUGS a. Thiazides b. Vitamin D 2. Malignancy 3. Primary hyperparathyroidism Management - Mild symptoms: PO calcium - Kidney disease: alfacalcidol - Severe symptoms: 10ml 10% calcium gluconate - Monitor patient with ECG Management 1. Correct dehydration 2. Bisphosphonates e.g.: 60 mg pamidronate infusion 3. Furosemide (although dehydration may worsen hypercalcaemia!) 4. Monitor patient with ECG 5. Early involvement of endocrine team Please note: these resources are copyright of the authors and OSCE-Aid unless otherwise stated. Please refer to our website terms & conditions at: http://www.osceaid.co.uk/terms&conditions.php. All resources can be printed and shared for personal use only. No amendment or alteration to these resources is allowed, unless otherwise agreed by the OSCE-Aid team. For any queries, please contact the team at: contact@osce-aid.co.uk. © 2016 www.osce-aid.co.uk