Zheng_Andrew_Diagnosis Symptoms Rabies
advertisement

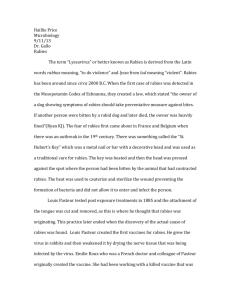
Radical Rabies: An Investigation on the Diagnosis, Signs, and Symptoms of Classical Rabies Virus Abstract Word Count: 97 Page Count: 6 Andrew Zheng Biomedical Sciences: Cluster 7 Dr. L and Master Dockter July 27, 2015 Abstract: Viruses are cunning. They manage to infiltrate every living thing and are able manipulate the cells within to duplicate. There are all sort of viruses but one extremely shrewd and calculating one is rabies. It travels up to the brain and completely annihilates the nervous system. There are still no tests to diagnosis rabies in humans before the onset of clinical disease. There are still no reliable cures to rabies. Yet, the symptoms of rabies are obvious and flagrant. Rabies can be horrifying to perceive but there must be more awareness to end the sequence of infection. Investigation: The realization of viruses occurred in the late 1880s, a reasonably short time ago, but viral diseases have morphed the past and evolution of life on this planet as long as they have existed. As far as we know, all living organisms can potentially become infected by viruses (J. Strauss and E. Strauss 1). Viruses infringe healthy cells and use them as hosts to replicate, so they can definitely be serious threats to animal and human health (Mandal). Even though progress in controlling infectious diseases has improved through upgraded sanitation, safer water supplies, the development of vaccines and antibiotics, and better medical care, viruses still roam everywhere (J. Strauss and E. Strauss 1). One virus that is in focus is rabies. The symptoms of rabies are threatening and lethal, and the diagnosis of the virus before it reaches the brain is crucial (J. Strauss and E. Strauss 144). Rabies is a uniformly fatal disease in mammals and humans, and has been known since the twenty-third century B.C. (J. Strauss and E. Strauss 144). It is a zoonotic disease, as it is present in the saliva of a rabid animal and is transmitted to humans through its bite. Infection begins by the tissues around the bite (“Rabies”). Without any response or treatment, the virus may travel up to the brain. Replication of the virus there leads to rabies (J. Strauss and E. Strauss 144). The probability that rabies will develop following a rabid animal’s bite depends on the location of the bite, the animal’s species, and the virus strain. For example, bites on the face and head resulted in rabies in 40-80% of human cases, whereas bites on the legs caused only 0-10% of people to become infected. The incubation period of symptomatic rabies can vary from less than a week to several years. In humans, rabies can be paralytic or may result in nonspecific neurological symptoms such as anxiety, agitation, and delirium. Biting others is not a consequence of human rabies and human-to-human transmission does not occur (J. Strauss and E. Strauss 144). The diagnosis of rabies in animals can be made after the detection of rabies from any area of an affected brain. However, in order to rule out rabies, the test must include tissues from two areas of the brain, preferably the brain stem and cerebellum. The test also requires the animal to be euthanized. The test takes around two hours but the time to ship the brain samples to a state public health or veterinary diagnostic laboratory for diagnosis may take several days (“Diagnosis”). On the other hand, diagnosing rabies in humans requires a plethora of tests; no single test is sufficient enough. “Tests are preformed from samples of saliva, serum, spinal fluid, and skin biopsies of hair follicles at the nape of the neck. Saliva can be tested by virus isolation or reverse transcription followed by polymerase chain reaction (RT-PCR). Serum and spinal fluid are tested for antibodies to rabies virus. Skin biopsy specimens are examined for rabies antigen in the cutaneous nerves at the base of hair follicles” (“Diagnosis”). More diagnosis techniques incorporate direct fluorescent antibody tests, histologic examinations, immunohistochemistry, electron microscopy, and amplification methods. The direct fluorescent antibody test (dFA) is based on the observation of rabies virus proteins (antigens) present in the tissues of a rabid animal. The ideal tissue for the test would be from the brain, since rabies is present in nervous tissues and not the blood like most viruses. The test works by incubating fluorescently-labeled anti-rabies antibodies with rabies-suspected brain tissue. The two would then bind together. Unbound antibodies could be washed away whereas bound ones would be visualized as fluorescent-apple-green areas. If the rabies virus is absent, then there would be no staining (e.g. see fig. 1) (“Diagnosis”). Fig. 1 Positive dFA Negative dFA http://www.cdc.gov/rabies/diagnosis/direct_fluorescent_antibody.html Histologic examination of biopsy or autopsy (post-mortem) tissues is sporadically useful in diagnosing rabies in unsuspected animals that have not been tested by routine methods. When brain tissue from rabies virus infected animals are stained with histologic stains such as hematoxylin and eosin, evidence of encephalomyelitis may be documented by a trained microscopist. Immunohistochemistry methods for the detection of rabies provide sensitive and specific means to discover rabies in formalin-fixed tissues. These methods are essentially more sensitive than histologic staining methods (“Diagnosis”). Electron microscopy can study the ultrastructure of viruses. Using this method, detailed observation of the structural components of viruses and their inclusions is possible. Rabies virus is in the family of Rhabdoviruses. Rhabdoviruses seem like bullet-shaped particles underneath an electron microscope (e.g. see fig. 2) (“Diagnosis”). “Negatively stained Rhabdovirus as seen through an electron microscope. Notice the bullet shape of the virus (A). See the ‘beehive’ like striations of the RNP (B). Notice the glycoprotein spikes in the outer member bilayer (C).” Fig. 2 http://www.cdc.gov/rabies/diagnosis/electron_microscopy.html Samples that contain very small amounts of rabies virus may be problematic to confirm as rabies-positive by customary approaches. Virus isolation in cell cultures increases the concentration of the virus. This is due to replication. Mouse neuroblastoma cells (MNA) and baby hamster kidney cells (BHK) provide an excellent and ideal environment for the amplification of rabies virus (“Diagnosis”). The development of clinical rabies in humans is divided into three general stages: the prodromal period, an acute neurologic phase, and coma preceding death. The prodromal period lasts from two to ten days and during that time, symptoms are usually mild and nonspecific. Some symptoms consist of general malaise, chills, fever, headache, photophobia (light sensitivity), anorexia, nausea, vomiting, diarrhea, sore throat, cough, and musculoskeletal pain. One peculiar early symptom though is abnormal sensation around the bite wound. The site might itch, burn, be numb, or have some sort of paresthesia (1: 914). During the acute neurologic phase, patients will exhibit signs of nervous system dysfunction. Anxiety, agitation, dysphagia (difficulty or discomfort swallowing), hypersalivation (the excess production of saliva), paralysis, and delirium are just some signs that would ensue. Occasionally, priapism, persistent and painful erections of the penis, or increased libido (sex drive) may be observed. Cases in which hyperactivity is predominant are categorized as furious rabies cases. When paralysis is prevalent, it is classified as paralytic or dumb rabies (1: 914). The percent of patients exhibiting hydrophobia, the fear of water, range from 17% to 80%. Hydrophobia is a pathognomonic sign of rabies believed to be caused by an amplified respiratory tract protective reflex. Hydrophobic episodes can actually last from one to five minutes and are triggered by attempts to drink. “In furious rabies, the neurologic period ends after 2 to 7 days with coma or sudden death from respiratory or cardiac arrest” (1: 914). Paralytic rabies occurs in about 20% of patients. This type of rabies may be more frequent in persons exposed to certain strains. One example is the vampire bat RABV. Again, patients will initially develop paresthesia and weakness, and finally flaccid paralysis. Paralysis then proceeds to paraplegia (impairment of motor skills in the lower body) and quadriplegia (disability in all the limbs). In paralytic rabies, the course to death is not exceedingly progressive. Some patients live up to thirty days with intensive care. Lastly, the final stage of this disease is coma, which lasts three to seven days and results in death. Patients that received respiratory assistance had their lives prolonged for several weeks (1: 914-915). To date, six cases of human recovery from clinical rabies have actually been documented. Five of the cases had exposures to animal bites while the other case was due to suspected inhalation of rabies virus in the laboratory. Only one of the patients had never been vaccinated and was set up in an experimental treatment. The trial included induction of ketamine coma in conjunction with antiviral compounds and demanding care. “Nevertheless, more than 10 attempts to repeat such experimental treatment (although with deviations and modifications) failed. However, in one vaccination failure case (immunoglobulin was not administered, although all five doses of vaccine were administered on time), the experimental treatment was implanted successfully. In addition, this was the only survival case where the virus variant was identified (vampire bat RABV)” (1: 915). Clinical disease in animals is very similar to that of humans, excluding the absence of hydrophobia. Signs can vary but can comprise of altered phonation (creating certain sounds through the vocal cords by quasi-periodic vibration), pica (tendency to crave abnormal foods), cranial nerve deficits, distorted activity patterns, and the loss of fear toward humans (1: 915). Conclusion: Rabies is appalling. The diagnosis process is insufficient and delayed. The symptoms are remarkably detrimental and disheartening. There is no remedy to cure rabies (although there are injections that need to be administered instantaneously after infection to prevent the virus from reaching the central nervous system). Rabies cannot be found clearly before it enters the brain, and cannot be extinguished after it enters the brain, so it is clear that it is perilous on all levels. Infection causes tens of thousands of deaths per year, especially in Asia and Africa. “40% of people who are bitten by suspect rabid animals are children under 15 years of age” (“Rabies”). Rabies cases must be eliminated around the world. Numerous people are at risk and vaccines can avert the towering figures. Rabies can and will be stopped with awareness and understanding. Works Cited "Diagnosis." Centers for Disease Control and Prevention. Centers for Disease Control and Prevention, 20 Sept. 2011. Web. 26 July 2015. "Diseases and Conditions: Rabies." Mayo Clinic. Mayo Clinic Staff, n.d. Web. 26 July 2015. Knipe, David M., PhD, and Peter M. Howley, MD. Fields Virology. 6th ed. Vol. 1. Philadelphia: Lippincott Williams & Wilkins, 2013. Print. Mandal, Ananya, MD. "What Is a Virus?" News Medical. News Medical, 09 Jan. 2010. Web. 26 July 2015. "Rabies." World Health Organization. WHO, 2015. Web. 25 July 2015. Strauss, James H., and Ellen G. Strauss. Viruses and Human Disease. 2nd ed. N.p.: Academic, 2008. Print.