Toward Integrated Laser-Driven Ion Accelerator Systems at the

Toward Integrated Laser-Driven Ion Accelerator
Systems at the Photo-Medical Research Center in
Japan
Abstract
P.R. Bolton 1 , T. Hori 1 , H. Kiriyama 1 , M. Mori 1 , H. Sakaki 1 ,
K. Sutherland 2 , M. Suzuki 1 , J. Wu 3 and A. Yogo 1
1 Photo-Medical Research Center, Japan Atomic Energy Agency,,
8-1-7 Umemidai Kizugawa-shi, Kyoto 619-0215 Japan
2 Hokkaido University, School of Medicine, Sapporo-shi Kita-ku Kita
12 Jo Nishi 5 Chome, 060-0812 Japan
3 SLAC National Accelerator Laboratory, Stanford University,
Menlo Park, California USA
Goals and early progress at the Photo-Medical Research Center are summarized. Laser-driven ion beam radiotherapy can require compact repetition-rated laser systems with peak powers approaching the PW level. Laser development at PMRC is outlined. Our parallel experimental and simulation efforts aimed at the development of a prototype ion beamline as an integrated laser-driven ion accelerator system are presented. In addition some of our first medical and radiobiological experimental investigations, proton-induced double strand breaking in human cancer cells and simulations of optimum dose distributions for ocular melanoma are discussed.
Recommended components of a balanced and comprehensive PMRC agenda are given.
1
1. Introduction
The case for ion beam radiotherapy continues to be well-made around the world. Globally the number of proton treatment facilities (PTFs), including those under development, is about thirty. Thousands of patients each year now receive proton beam radiotherapy for treatment of cancerous tumors. The well-known Bragg peak phenomenon enables improved depth localization of deposited proton dose where the depth of the so-called ‘Bragg peak’ increases with the proton kinetic energy. It was highlighted by Wilson years ago that adequate dose localization can spare healthy tissue that can surround a cancerous tumor [1]. This is an artifact of the inverse energy dependence of the proton stopping power in contrast to the exponential dose reduction
(the exception being close to the surface) with increasing depth for x-ray photons.
Professor Abe has written “It is no exaggeration to say that the history of radiotherapy is the history of struggling to improve the dose localization and cell killing effects of radiation” [2]. Our flagship theme and main goal at the Photo-Medical Research Center
(PMRC) is to develop a compact ion beam radiotherapy (IBRT) facility that is laser-driven (L-IBRT). In this report the term ion is inclusive of protons. The Bragg peak phenomenon indicates that shallower (more superficial) tumors can be treated with lower ion energy than deeper ones (for example, the 40-60 MeV proton energy
2
requirement for ocular melanoma [3]). A small tumor requires fewer protons to achieve a given integrated dose level. Our initial goal will then focus where possible on the treatment of small and superficial tumors (in many cases early stage tumors).
PMRC was established in 2007 as a community-based, multidisciplinary research and development hub to foster and promote collaboration and cooperation with industrial, academic, medical, institutional and government partners aimed at the targeted innovation of medical and related photonics technologies. PMRC is funded by the Japan Atomic Energy Agency (JAEA – through the ‘Special Coordination Fund
(SCF) for Promoting Science and Technology as commissioned by the Japan Ministry of Education, Culture, Sports, Science and Technology (MEXT)) and also by its ten funding partners.
This proceedings report presents a brief summary of some of the important activities at PMRC that are aimed at development of a prototype ion beamline that is compact and laser-driven for application to cancer radiotherapy (an L-IBRT facility).
2. Laser Requirements for Ion Acceleration
The transverse normal sheath acceleration model (typically applied to thicker targets) has become well-known and is relevant up to intensities near 10
21
W/cm
2
[4].
3
Also, for ultrashort pulses and ultrathin foil targets a theory of coherent ion acceleration has been recently reported [5]. Higher peak intensities (10
22 to 10
24
W/cm
2
) are appropriate to the radiation pressure (laser piston) regime [6]. These models describe charge separation driven by highly intense (relativistic) laser pulses. To date most experimental results can be characterized with the following ‘at source’ features that are can be well-predicted by the TNSA model because of the target thickness and laser pulse durations used: divergent, laminar proton spray: large angular spread ~ 10 degrees or more ultralow emittance ~ 10
-4
mm mrad (transverse) high extraction field: ~ TV/m level high peak current: bunch charge ~ 1 - 100’s nC short bunch duration ~ picoseconds large energy spread with a maximum value: spread ~ 100 % intensity dependent cutoff value significant background particles: electrons, other ions, x-rays…
At the J-KAREN facility of the Kansai Photon Science Institute (KPSI) we
4
have recently reached cutoff proton energies near 7 MeV with 1.8 J (51 TW) focused to about 10
20
W/cm
2
onto a 2.5 micron stainless steel foil target. In general experimental observations to date make it clear that the acceleration of protons by lasers to cutoff energies near 100 MeV will require that laser systems deliver peak powers in the
100’s TW to 1 PW range to targets. For a 100 fsec pulse duration this means pulse energies of 10’s to 100 J delivered at a repetition-rate (~ 10 Hz - 100 Hz) and focused to intensities of order 10
21
W/cm
2
. Peak power alone is not adequate. Pulses need to be
‘clean’ in the sense of having very high contrast (at least ~ 10 -10
) and stable on a shot-to-shot basis. Finally, we insist, that to provide a laser-driven ion beam radiotherapy (L-IBRT) facility which is cheaper and more compact than a conventional
IBRT facility (such as a synchrotron-based one), such a laser system also must be compact.
3. Summary of Laser Development at PMRC
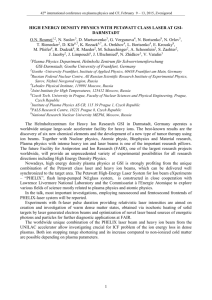
The J-KAREN laser at the Kansai Photon Science Institute of JAEA, (a schematic of which is shown in figure 1), is used for PMRC studies of ion yields in high power and high intensity laser experiments. It is a Ti:Sapphire-based double CPA system with a two stage OPCPA preamplifier that precedes a series of higher power multi-pass amplifiers where the second one is cryogenically cooled [7,8]. The system
5
bandwidth is capable of generating 30-40 fsec compressed pulses with a contrast as good as 10
-10
. Furthermore, this has recently been improved. A three-pass Ti:sapphire booster amplifier has been added this year to the system which will enable ~ 0.5 PW operation (20 J in 38 fsec). The booster amplifier is pumped by ~ 60 J of second harmonic emission from a Nd:glass laser for which the ir extraction efficiency is near
50 %. At this pump energy we anticipate one shot approximately every 20 minutes.
The pump beam profile at the Ti:sapphire crystal of the booster amplifier is made uniform with a diffractive optical element (homogenizer) by SILIOS Technologies [9].
With increased peak power from J-KAREN laser system we hope to reach focused irradiation levels near 10
21
W/cm
2
on target.
In collaboration with one of our PMRC partners we are also developing a more compact (tabletop) solid state system that is designed to operate at a repetition rate up to
100 Hz (currently at 10 Hz) with laser diode pumping. This is a CPA configuration with a BBO-based three stage OPCPA preamplifier (currently pumped with 532 nm emission from a Nd:YAG laser) and an Yb:YAG thin disk final amplifier (laser diode pumped at 940nm) [10]. The system starts with a broadband, diode pumped, mode-locked Yb:YAG oscillator operating at a central wavelength of 1030 nm at 38 mW of average power (0.47 nJ at 80 MHz). The Yb:YAG material is known for its
6
low quantum defect which can significantly reduce thermal loading and the emission bandwidth is broad enough (with a quasi-flat-topped spectral profile) to support compressed femtosecond pulse of duration (FWHM), 250 - 300 fsec.
The OPCPA single pass gain is ~ 10
7 bringing the ir pulse energy to 6.5 mJ as a stretched seed for the thin disk power amplifier. With diode pumping of the Yb:YAG disk we have reached 70 mJ (uncompressed). With the 10.8 nm bandwidth pulses we have demonstrated compression to a duration of about 230 fsec (near transform limit).
We aim to reach 200 mJ (uncompressed) soon which will represent 0.6 TW of peak power (with a 70 % compressor efficiency).
4. Integrated Laser-Driven Ion Accelerator System (ILDIAS)
As stated in section 2, the ‘spray’ of ions driven from the target rear surface is well-organized and the 10
-4
level emittance is orders of magnitude lower than that of a conventional accelerator ion source. However the angular divergence of this emission and the typically large energy spread are two serious challenges that must be confronted in the development of a laser-driven ion beamline for cancer therapy. Ion emission features (especially the energy spectrum, the single bunch charge and associated energy efficiency) are strongly dependent on the laser pulse parameters so the ion beamline is
7
appropriately considered as part of an integrated laser-driven ion accelerator system
(ILDIAS). The ILDIAS concept brings a systems approach to L-IBRT development where diagnostics and beam control functions are addressed in addition to beamline and ion optics designs. We necessarily include also the laser and the laser target (the photo-anode ion source) development in the ILDIAS concept. The laser not only accelerates ions but can provide synchronous probe pulses for beamline diagnostics and controls. So, in addition to laser development we must also develop clean ion beamlines
(without background xrays, neutrons, and other unwanted ions) with adequate shielding, focusing, collimation, steering, fast-shuttering, instrumentation and controls for stability, etc. ILDIAS is therefore defined to include all ion ‘transport’ which we distinguish from the ion ‘delivery’ system. Ion delivery is downstream of ion transport and deals with the patient/tumor specific aspects of the final beam delivery to the patient which includes a gantry (where needed), dosimetry, final collimation, spot-scanning and organ motion tracking for example.
An initial demonstration of 2 MeV proton focusing was made at PMRC by
Nishiuchi-san and co-workers [11]. This effort was conducted at a 1 Hz repetition rate using a moving polyimide tape target (of 12.5 micron thickness) and used a pair of conventional permanent quadrupole magnets (that were designed for 0.5 MeV protons).
8
With the J-KAREN laser pulse focused to intensities up to 10
20
W/cm
2
(and a contrast of 10
-7
at ~100 psec prior to the peak of the main pulse) onto the tape target a broad proton spectrum with a 3 MeV cutoff was generated. This was determined with an inline time-of-flight spectrometer based on detection of proton-induced scintillation that was positioned about 1.9 meters from the tape target. CR-39 film tracks were used to determined the +/- 10 degree divergence from the tape source and also in the focal plane have verified focusing to a 3 mm x 8 mm spot located 650 mm from the tape target.
Within the a 200 KeV energy spread centered at 2.4 MeV a single proton bunch contained 1.3 x 10
7
protons of which about 30 % were estimated to reach the focal plane according to a Monte Carlo simulation. The transmission of the PMQ pair relative to the full proton spectrum is only about 3 %.
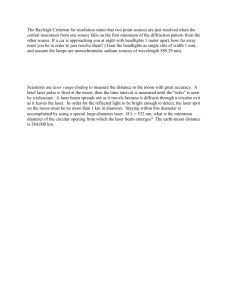
In parallel with these experimental tests we have also been simulating beamline transport with candidate designs. Figure 2 illustrates a test beamline conceptual design shown with a compact laser and embedded within a simplified gantry. A summary of simulation input parameters is given here. The laser target/ ion source generates a 1 nC proton bunch for each laser shot with an energy spread near 100 % , a beam divergence of +/- 5 degrees and a cut-off energy of 80 MeV. The beamline is designed for 55 MeV protons such that the overall proton transmission (to the patient as shown in the figure)
9
is about 1.2 % and the transmitted energy spread is only about 1.3 %. The 55 MeV was chosen with treatment of ocular melanoma in mind. Dose simulations for ocular melanoma performed at Hokkaido University will be shown in section V (discussion of integrated dose as well as laser pulse and bunch charge requirements associated with the simulation will be included in this latter section). With such designs most of the laser-accelerated protons are still discarded due to the large divergence and energy spread at the source. The effective laser-to-proton energy efficiency is then the product of the laser-to-proton energy efficiency at the source (which can be up to a few %) and the proton beamline transmission to the tumor. This effective efficiency is then of order
10
-4
to 10
-3
. We can ultimately deliver more laser-accelerated protons to the tumor
(higher effective efficiency) if the at source divergence and energy spread can be significantly reduced. Consequently increasing the effective energy efficiency is a challenge for targetry as much as it is for beamline optics.
ILDIAS development requires the sustained coordinated efforts of the medical, laser, laser-plasma and accelerator communities over an extended time. It is initially limited by laser and target technology yet must be guided by rigorous medical requirements. Repetition-rated targetry is a major challenge and is an integral part of this systems approach. The target provides both the photo-anode and extraction field for
10
accelerating ions. Test beamline development with the ILDIAS concept is consistent with a ‘shakedown’ philosophy in which we seek to know as quickly as possible what main technical challenges and difficulties to expect.
5. Medical Applications
The ILDIAS conceptual design and parameters discussed in section 4 are based on the results of dose distribution simulations reported by Sutherland and co-workers
[3]. The spread out Bragg peak (SOBP) is simulated by a weighted summation of five discrete central values of proton beam energy. In this work the diameter (few mm) and energy spread (few percent) of an ideal pencil proton beam were varied to obtain optimally uniform dose distributions. Simulated dose distributions in the case of ocular melanoma reveal that the sensitivity of dose to surrounding tissue (organs at risk
– OAR) to proton beam diameter and energy spread exceeds that of the tumor being treated. The required proton energy spectrum for optimized dose distributions spans 40 to 60 MeV requiring a total of about 2 x 10
10
protons to reach an integrated dose of 55
Gy for a tumor mass near 750 mg. This integrated dose level can be obtained with a laser-driven proton source that delivers 10
6
protons per laser pulse to the tumor at a 10
Hz repetition-rate extended over twenty fractions each of duration two minutes.
11
Spot-scanning requires precise control of the parameters of a well-specified pencil proton beam such as energy, position and integration time to a specified spot dose level.
The beam diameter and its lateral displacement in the scan will also determine the minimally relevant tumor size.
There is interest in investigating the potential application of PET imaging using radioactive isotopes in an autonomous mode. Detection of gamma photons following positron emission from proton-induced short-lived isotopes such as
11
C (decay half life
~ 20 minutes) and
15
O (decay half life ~ 2 minutes) would be implemented. Some preliminary measurements have been conducted at the Hyogo Ion Beam Medical Center
(HIBMC – a PMRC partner) to characterize how well the proton beam position could be monitored using water (ice), lucite and polyethylene targets [12]. The phantoms were irradiated with a 5 mm diameter proton beam of 80 MeV kinetic energy to an integrated proton number of order 10
10
( ~ 5 minute proton irradiation time).
Spot-scanning was also used with ~ 2 mm beam spacings. It is important to demonstrate that an autonomous PET technique can be used to measure proton dose distributions in small tumors, with short proton irradiation times and with adequately short PET scan times.
For example, it remains a challenge to obtain clear PET images following irradiation at the reduced level of 10
9
protons.
12
With the same moving tape target as described in section 4 protons in the energy range 0.8 to 2.4 MeV were used to irradiate human cancer cells in vacuum [13].
The proton yield was generated by a laser intensity of about 5 x 10
19
W/cm
2 on target delivered at a 1 Hz repetition rate. An integrated proton dose of 20 Gy was delivered to the cells with 200 proton bunches of duration about 15 nsec (one proton bunch per laser pulse). At the cell site the proton irradiation level was estimated to be about 10
3 nsec
-1 mm
-1
. We demonstrated for the first time laser-driven proton-induced double strand breaking in human cancer cells (A549).
6. Closing Remarks
Because of its multidisciplinary nature PMRC is a multifaceted effort with its own intrinsic complexity. It is important to pursue this mission with a balance of multiple parallel paths or foci where the portion of effort and relative significance for each path or focus will vary with time as our program matures. The first path which is immediately critical is clearly the continued development of highest peak power laser systems (such as J-KAREN) and laser-plasma experiments using them to explore and determine laser pulse, target and diagnostic requirements in the single shot mode. A second parallel path, also immediately critical, is the development and application of a
13
more compact repetition-rated laser system. A repetition-rated system can also be used to advance targetry where the repetition-rated feature is essential. However, as targets become more sophisticated the challenge of 10 Hz to 100 Hz operation increases.
A third parallel path is the development of a laser-driven prototype ion beamline that demonstrates medically acceptable performance at a clinical stage as a step toward the L-IBRT clinical facility. This has been referred to as the integrated laser-driven ion accelerator system or ILDIAS in which we take a systems approach integrating the laser system and targetry with ion beamline design. This part of the beamline is the ion transport line for which we must address ion optics (that are tunable as well as unique to the high peak currents and divergence at the ion source), beam diagnostics, dosimetry (with the required redundancies) and potential beam controls
(including the potential for laser control of ion beam parameters and fast shutter capability). Toward realizing the medical prototype, as an intermediate step, it is important develop a lower energy ‘test’ ion beamline as a focus for initial ILDIAS developments. This is partially due to the fact lower laser peak powers and therefore proton energies will be available first. Furthermore, a test beamline can also serve a dual use in supporting a medical and nonmedical agenda for science and applications at the reduced ion energy. This path is also about maintaining a ‘state-of-readiness’ for when
14
we do have repetition-rated laser pulses that can generate beams of protons with adequately high proton energies. During this shakedown process we learn about where the main technical challenges are in this endeavour. The ILDIAS path will become increasing important in the PMRC program. In particular the compactness requirement must be addressed with rigor following the demonstration of medically acceptable performance at the higher energy (the clinical medical prototype). The design of downstream beam delivery components such as a gantry (if needed) and a spot-scanning system (if needed) will depend critically on making the ion transport beamline
‘optimally’ compact through appropriate engineering and design.
A fourth parallel path is the focus on medical/biological studies relevant to laser-driven ion beams. This path is critical because we are guided by medical requirements in all phases of PMRC. There are many essential topics in this path that must be pursued in a timely manner. For example, therapy ‘niche’ verification is to be determined by available ion beam energy, flux and other performance capabilities.
The development of appropriate imaging techniques must be medically guided toward the ultimate goal of ‘image-guided’ therapy. It is well-known that ion beam irradiation studies that focus on the dynamics of the short ion bunch are essential to determine
15
relative biological efficiency for single cells and tissue. In the conventional longer bunch/pulse mode experimental comparisons are being made with protons, carbon ions and x-rays at the HIBMC [14]. It is clear also that detailed quantitative evaluations are needed with dose distribution simulations, the unique role for positron emission tomography (PET) for short irradiation fractions with low doses and small tumors, spot-scanning requirements and treatment planning issues in general. As importantly this path provides the much needed channel for ‘bottom line’ medical guidance and specification of performance requirements for a ‘test’ beamline and ultimately for the clinical L-IBRT facility.
Finally it is important to also establish as a fifth parallel path, a nonmedical science and technology path where we can achieve mid-program milestone successes that mark our progress and support the case for the overall mission of developing an
L-IBRT facility while also developing a research and development hub for advancing photo-medical technology. For this path lower energy ‘test’ ion beamline development can be important. It has already been noted above that identified medical and radiobiological studies can also be conducted on such a test beamline.
L-IBRT is still high risk and exploratory. As has been shown in many other technological fields over the past few decades, the ubiquitous laser will find its
16
relevance in IBRT and so we must proceed along this provocative and ambitious trail.
Of the five parallel paths identified above it is ILDIAS (third path) and the medical/biological studies (fourth path) which represent critical ‘next steps’ toward
L-IBRT development. The paths that are critically immediate are the first two, the development of adequate lasers and laser-plasma experiments using high peak power single shot and repetition-rated systems. As we proceed in a parallel arrangement as recommended here we must also be mindful of two ongoing global surveys: (i) ion yield results (notably spectra and efficiencies) from other high power laser facilities around the world noting laser pulse requirements, diagnostics and target types used in relevant best cases and (ii) an assessment of existing (often called classical or conventional)
IBRT facilities as well as those under development, funded for future development and newly proposed. The former survey clarifies latest progress and capability with ion source development for L-IBRT and the latter clarifies the state-of-the-art for IBRT which we must match and which we aim to advance.
17
ACKNOWLEDGEMENTS
This work was supported by the Special Coordination Fund (SCF) for Promoting
Science and Technology as commissioned by the Ministry of Education, Culture, Sports,
Science and Technology (MEXT) of Japan and also by the funding partners of the
Photo-Medical Research Center (PMRC).
References
[1] R.R. Wilson, Radiol. 47 (1946) 487.
[2] M. Abe, Proc. Japan. Acad. Ser B 83 (2007) 151.
[3] K. Sutherland, S. Miyajijma, H. Date, H. Shirato, M. Ishikawa, M. Murakami, M.
Yamagiwa, P.R. Bolton and T. Tajima, Radiol. Phys. and Technol. in press (2009).
[4] S. C. Wilks, A.B. Langdon, T.E. Cowan, M. Roth, M. Singh, S. Hatchett, M.H.
Key, D. Pennington, A. MacKinnon and R.A. Snavely, Phys. of Plasma. 8
(2001) 542.
[5] T. Tajima, D. Habs and X. Yan, Rev of Accel. Sci. and Tech. (RAST) 1 (2009) 1.
[6] T. Esirkepov, M. Borghesi, S.V. Bulanov, G. Mourou and T. Tajima,
Phys. Rev. Lett. 92 (2004) 175003.
[7] H. Kiriyama, M. Mori, Y. Nakai, T. Shimomura, M. Tanoue, A. Akutsu, S. Kondo, S.
18
Kanazawa, H. Okada, T. Motomura, H. Daido, T. Kimura and T. Tajima, Opt Lett.
33 (2008) 645
[8] H. Kiriyama, M. Mori, Y. Nakai, T. Shimomura, M. Tanoue, A. Akutsu, H. Okada, T.
Motomura, S. Kondo, S. Kanazawa, A. Sagisaka, J. Ma, I. Daito, H. Kotaki, H.
Daido, S. Bulanov, T. Kimura and T. Tajima, Opt. Comm. 282 (2009) 625.
[9] K. Ertel, C. Hooker, S.J. Hawkes, B.T. Parry and J. Collier,
Opt. Exp. 16 (2008) 8039.
[10] M. Suzuki, H. Kiriyama, I. Daito, H. Okada, Y. Nakai, S. Orimo, M. Sato,
Y. Tamaoki, T. Yoshii, J. Maeda, S. Matsuoka, H. Kan, P.R. Bolton, H. Daido
and S. Kawanishi, Appl. Phys. B (Rapid Communication), in press (2009).
[11] M. Nishiuchi, I. Daito, M. Ikegami, H. Daido, M. Mori, S. Orimo, K. Ogura,
A.
Sagisaka, A. Yogo, A.S. Pirozhkov, H. Sugiyama, H. Kiriyama, H. Okada,
S. Kanazawa, S. Kondo, T. Shimomura, M. Tanoue, Y. Nakai, H. Sasao,
D. Wakai, H. Sakaki, P.R. Bolton, I.W. Choi, J.H. Sung, J. Lee, Y. Oishi, T. Fujii,
K. Nemoto, H. Souda, A. Noda, Y. Iseki and T. Yoshiyuki , Appl. Phys. Lett. 94
(2009) 061107.
[12] T. Maeda, private communication
19
[13] A. Yogo, K. Sato, M. Nishikino, M. Mori, T. Teshima, H. Numasaki,
M. Murakami, Y. Demizu, S. Akagi, S. Nagayama, K. Ogura, A. Sagisaka, S. Orimo,
M. Nishiuchi, A.S. Pirozhkov, M. Ikegami, M. Tampo, H. Sakaki, M. Suzuki,
I. Daito, Y. Oishi, H. Sugiyama, H. Kiriyama, H. Okada, S. Kanazawa, S. Kondo,
T. Shimomura, Y. Nakai, M. Tanoue, H. Sasao, D. Wakai, P.R. Bolton and
H. Daido, Appl. Phys. Lett. 94 (2009) 181502.
[14] T. Akagi – private communication
20
Figure captions
Fig. 1. Architecture of the J-KAREN laser at the Kansai Photon Science Institute
(KPSI)
Fig. 2. Concept of a laser-accelerated double bend achromat ion transport line within a gantry.
21
Figure 1
22
Figure 2
23