To perceive a sensation Stimulation must be strong enough to
advertisement

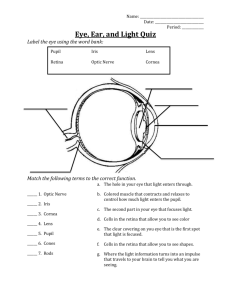
To perceive a sensation Stimulation must be strong enough to initiate response Receptor must convert stimulus to impulse Interpretation of impulse must occur in brain Receptors Cells that receive information from the environment & then send impulses via conductors to CNS Converts stimulus to impulse Sensory Categories Somatic receptors- in skin, muscles & joints Visceral receptors- in internal organs Special sense receptors- in head Types of receptors Photoreceptors- sensitive to light stimuli Chemoreceptors- sensitive to chemical stimuli Mechanoreceptors- sensitive to movement Sense organs receive stimulation & receptor converts stimulus into electrical impulse that is sent to specific region of brain All impulses generated by different sense organs are electrically similar but region of brain where they go varies depending on which brain lobe is in charge of those stimuli Taste & Smell Special chemoreceptors allow for senses of taste & smell Taste buds- clusters of chemoreceptors for taste; found on tongue, roof of mouth & in throat Papillae- small projections on tongue that house most of the 10,000 taste buds; gives tongue velvet-like appearance Substance must be in solution before its flavor can be detected Solution enters taste buds through small opening & stimulates nerve endings that line inner surface Nerve endings begin impulse that travels to parietal lobe of brain to be interpreted as taste Humans detect salt, sweet, sour & bitter flavors Other flavors perceived by receptors in nasal passages & as result of smelling food rather than tasting them Olfactory receptors- ciliated chemoreceptors located in olfactory epithelium of nasal passage; lie within mucus lining; short life span (~60 days) Special olfactory receptors respond to different chemicals Chemicals as gas or particles enter nose & dissolve in watery mucus before they stimulate olfactory receptors Olfactory receptors generate impulses that travel through olfactory nerve to temporal lobe Sight Wall of eyeball has 3 layers Sclera- sclerotic coat Outer layer of white opaque tough fibrous membrane Helps maintain shape Forms transparent cornea where the light waves pass into the eyeball Cornea is extremely sensitive to touch so has many nerve endings but lacks blood vessels (this lack of blood vessels is why they can be transplanted) Uvea- middle layer of eye Choroid coat Supplies blood vessels (carry nutrients/wastes) to layers of eye Contains pigment granules that prevent reflection of light within eye & absorb stray light that would otherwise blur image Ciliary body Two smooth muscles that support & modify shape of lens Part of anterior chamber of eye Contraction of muscles causes light to bend more Iris Regulates amount of light entering eye Two muscle layers: sphincter (circular fibers which decrease size of pupil) & radiate (fibers which increase size of pupil) Papillary dilator muscles contract & allow more light into eye Colored portion of eye due to pigment found in muscle layers Back layer contains large granules of blue pigment & front layer will either have no pigment or contain melanin Eyes of all newborns are blue since it takes time for melanin to form Pupil Opening for light to enter eye Retina- innermost layer Completely lines inner surface & contains cells responsible for converting light into sensory impulses Vein-like structure is nerve ganglia Optic nerve leaves here to send messages to brain; blind spot results from lack of neurons where optic nerve leaves the eye Photoreceptor cells are sensitive to damage from heat/light Rods- nerve cells containing light sensitive molecules for vision in dim light Outer segment contains photosensitive chemical rhodopsin or visual purple; 120 million/retina; several rods share one neuron to brain; detect light in shades of gray Cones- conical shaped; responsible for color vision; 3 kinds- red (L), green (M), & blue (S); names of cones based on light wavelength; each cone contains photochemical substance sensitive to that wavelength; each cone has its own neuron to brain; 6 million/retina; sensitive to color & bright light; center of retina only has these while edges of retina contain mixture of rods/cones Visible color is produced by combining the various stimulations of cones in proper proportions & these signals are relayed to brain for color analysis to take place Lens- behind pupil & iris Disc shaped elastic & transparent Lacks blood vessels Held in place by ligament attached to ciliary muscle which controls amount of tension exerted on lens Job is to converge or focus light rays Vision is most acute when light rays focus on fovea centralis Only a limited part of the electromagnetic spectrum can excite our photoreceptors When light energy stimulates rods/cones, nerve impulses are produced/transmitted to visual center in occipital lobe of brain to be interpreted Photoreceptors are activated when light produces chemical change in pigment molecules in the receptor cells Lens focuses image on retina where image will always be upside down/reversed but brain corrects this Bright light dazzles eyes & causes pain because the intense light bleaches the rhodopsin Dark adaptation- rhodopsin must accumulate in rods for vision in dimmer light; gradually increases & max sensitivity is reached in 20 min Positive afterimage- carryover of visual impressions that are exactly the same as the original stimulus pattern; ex. Movie Negative afterimage- some visual image remains even though external stimulus has stopped; probably due to fatigue of originally stimulated receptors Some Disorders of Vision Astigmatism- caused by imperfect curvature of cornea or lens so light doesn’t come to a single sharp focal point on retina; eyestrain & headaches common; corrected by prescription lens Myopia- nearsightedness; image focuses in front of retina usually because eye is too long for refraction of lens; can see up close but not far away without help of concave lens to change focal point to fall on retina Hypermetropia- hyperopia; farsightedness; image focuses behind the retina because eye is too short for refraction of lens; can see near objects only with help of convex lens Presbyopia- ciliary muscles that change shape of lens lose their contractive power; eyeglasses are needed for reading; loss of elasticity of lens; common in individuals over 50 Colorblindness- deficiency in color perception; usually absence of red or green cones; may be inherited (8% of males) or result of injury or disease Monochromats- people who see only black/white; total colorblindness; rare; lack of cones or have defect in visual cortex of brain Dichromats- red/green or blue/yellow (rarer) colorblind due to problem in cone receptors or neurological confusion of colors; genes for M&L cones are found on X chromosome Trichromats- normal color vision Conjunctiviitis- pink eye; viral or bacterial infection; can be an allergic reaction, or due to chemical irritants or leaving contacts in too long; results in dilation of blood vessels in conjunctiva Cataracts- clouding of the normally transparent lens of eye; proteins in lens change shape & lens becomes cloudy; result from injury, heredity, birth defects, dehydration, cigarette smoking, sunlight exposure; can be surgically removed Glaucoma- increased fluid pressure within eye which can damage the optic nerve & cause gradual blindness; damage is irreversible but medication/surgery can help decrease pressure; degenerative disease; 2-3 million US afflicted; begins with decrease in peripheral vision; optic nerve enlarges & becomes assymetrical Retinal detachment- retina separates from back of eye which can lead to vision loss or blindness; common cause is shrinking of vitreous fluid in eye which is normal & expected with age; requires surgery & >90% can be repaired; torn retinas are treated by lasers or freezing to prevent detachment; nearsighted people at greater risk since retinal layer is thinner Macular degeneration- loss of clarity of vision in center of visual field; risk factors: age, smoking, genetic predisposition Hearing & Balance Ear Sensitive mechanical receptor capable of detecting physical movement of air in form of sound vibrations & converting them into neural signals sent to brain for interpretation External ear- pinna Outside lateral surface of head Made of flexible cartilage & skin Serves to gather sound waves into auditory canal which extends into temporal bone to tympanic membrane Ceruminous glands in auditory canal produce sticky earwax that keeps foreign objects out Middle ear Small airfilled chamber within temporal bone, walls lined by mucus membrane Ossicles Malleus attaches to inner surface of eardrum & incus Incus attaches to stapes Stapes base vibrates against membrane on inner wall of middle ear (oval window) Sound energy is concentrated/amplified here Carries sound waves from outer ear to inner ear Must maintain equal pressure between middle ear & outside or eardrum will not vibrate properly & hearing will be impaired If the outside pressure decreases, the middle ear pressure is higher than outside so the eardrum bulges outward; if the outside pressure increases, the middle ear pressure is lower than outside so the eardrum bulges inward Eustachian tube- tube leading from middle ear to pharynx that equalizes pressure between middle ear & outside Swallowing or yawning causes muscle to open throat opening of tube allowing air to move through it & equalize pressure Inner ear Bony labyrinth divided into 3 fluid filled canals, membranous labyrinth separated from body by liquid called perilymph & is filled by endolymph Vestibule- connects to middle ear by oval window, contains 2 fluid filled sacs which have hair cells in them; otoliths are small particles of calcium carbonate that entangle in the hairs Cochlea- snail shell which has branch of auditory nerve leaving its middle; oval window begins vibrations in fluid here; functional unit of hearing in inner ear Organ of Corti- sense receptors are cilia on columnar epithelium; movement of fluid stimulates cilia & initiates nerve impulses to auditory nerve; changes sound waves to nerve impulses How we hear Stapes transmits vibrations via oval window to fluid in vestibular canal Cilia in organ of Corti vibrate & waves pass on to cochlea Auditory nerve picks up impulses which travel to hearing center of temporal lobe of brain Conductive hearing loss occurs when a problem is in outer or middle ear; may result from blockage of external ear canal, perforated eardrum, impacted wax, otosclerosis or middle ear infection; usually corrected by surgery or hearing aid Nerve hearing impairment is when inner ear has problem; caused by disturbances in inner ear circulation or fluid pressure or from problems in nerve conduction; not correctable but rarely total deafness Semicircular canals 3 looped tubes each lying in a different plane In temporal bone Where canals meet there is a group of cilia that can detect changes in acceleration/deceleration Impulses go to medulla oblongata of brain Helps to maintain proper balance Static equilibrium- orientation of body relative to ground; when head tilts the otoliths in vestibule contact hair cells which send nerve impulses to brain Dynamic equilibrium- orientation of body in relation to movement along horizontal plane; when accelerating the fluid in semicircular canals cause cilia to bend in direction opposite to motion