Spondylolysis
advertisement

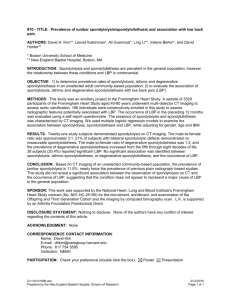
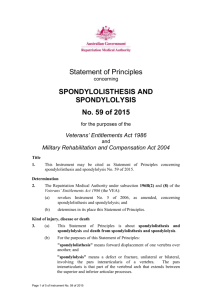
Spondylolysis What Is Spondylolysis? Spondylolysis results when cracks or fractures occur in the pars interarticularis, the portion of the lumbar spine that joins the upper and lower joints together of a single vertebra (individual bone in the spine). Spondylolysis is the middle of 3 stages of injury to the pars interarticularis, with the first (least serious) being a stress reaction and the third (most serious) being actual slippage of vertebra(e), or spondylolisthesis. In the vast majority of children, the pars interarticularis is normal. But certain patients begin to experience abnormal growth and development in the pars interarticularis, usually after age 8. In patients with spondylolysis, stress reaction or injury may occur with the excessive wear and tear from activities of daily living, sports, or a fall. Gymnastics and heavy weightlifting are particularly culpable aggravators of spondylolysis symptoms. Certain ethic groups, like Alaskan Indians, are prone to spondylolysis due to a genetic weakness to the bone. Symptoms As with any spine condition or deformity, symptoms can vary from patient to patient but generally include the following: • Persistent lower back pain • Stiffness in the back or legs • Hamstring muscle tightness. Diagnostics X-ray imaging typically confirms bony abnormality, particular in cases of spondylolysis and spondylolisthesis. However, with a stress reaction, an x-ray may not reveal any abnormality. Treatment The goals of treatment include relieving pain, decreasing acute spasm, and restoring spinal flexibility. The prognosis is affected by slippage of one vertebra on another (spondylolisthesis). Patients with less than 50% slippage tend to fare well through adolescence. With slippage of 50% or greater, the potential for additional slippage with growth and aging is greater. Nonoperative Treatment Most spondylolysis patients will respond well to conservative (nonoperative) medical management. Post-treatment “maintenance” exercises like truncal core muscle strengthening (pilates or yoga) may be prescribed to condition the muscles and minimize reinjury. • • • • (therapist will "crunches”) Anti-inflammatory drugs Brace wear Activity modifications Physical therapy treatment that incorporates truncal core strengthening exercises caution patient on avoiding hyperextension maneuvers and excessive abdominal Operative Treatment If the pain, spasm, or slippage increases despite conservative management, then the surgeon may discuss several potential surgical options with the patient: 1) Spinal fusion (for spondylolisthesis) For a majority of children and adults, fusing the fifth lumbar vertebra to the sacrum (the most common vertebrae involved in adolescents with spondylolisthesis) is the preferred surgical option. The fusion involves removing the loose bony fragments and placing bone graft that will lead to the 2 vertebrae “fusing together" to prevent any further slippage. Specially designed screws and rods may be needed to hold the vertebrae in place to help the two bones fuse together. A perforated, hollow cylinder called a “cage” is sometimes required. The “cage” is filled with bone matter and placed in the disc space between the two vertebrae to increase the likelihood of fusion. Bones may be realigned depending on how much one vertebra has slipped forward on the other. The most important steps are restoring stability and making sure the nerves have no pressure on them. 2) Pars repair At times the pars fracture can be repaired without fusing 2 vertebrae together. This involves removing any scar material that may have developed in thefracture site of a single vertebra, and stabilizing the 2 sides of the fracture to restore normal anatomy. Spondylolisthesis <separate menu link under Spondylolysis> Isthmic spondylolisthesis results when a fracture gap at the pars interarticularis (the junction of the upper and lower lumbar spine joints of one vertebra) widens. Widening of the gap leads to the fifth lumbar vertebra shifting forward on the part of the pelvic bone called the sacrum; this is known as “slippage.” Degenerative spondylolisthesis results when wear and tear breaks down the pars interarticularis, causing slippage of one vertebra on another. This is more common in adults and most commonly occurs between the fourth and fifth lumbar vertebrae. Symptoms The primary symptom is pain related to nerve root irritation, which can occur in the lower back, buttocks, or legs. Numbness or a tingling sensation of the legs Treatment Nonoperative Treatment Post-treatment “maintenance” exercises like truncal core muscle strengthening (pilates or yoga) may be prescribed to condition the muscles and minimize reinjury. • • Anti-inflammatory drugs Brace wear • Activity modifications • Physical therapy treatment that incorporates truncal core strengthening exercises (The therapist will caution the patient on avoiding hyperextension maneuvers and excessive abdominal "crunches”) Operative Treatment If the pain, spasm, or slippage increases despite conservative management, then the surgeon may discuss spinal fusion with the patient: For a majority of children and adults, fusing the fifth lumbar vertebra to the sacrum (the most common vertebrae involved in adolescents with spondylolisthesis) is the preferred surgical option. The fusion involves removing the loose bony fragments and placing bone graft that will lead to the 2 vertebrae “fusing together" to prevent any further slippage. Specially designed screws and rods may be needed to hold the vertebrae in place to help the two bones fuse together. A perforated, hollow cylinder called a “cage” is sometimes required. The “cage” is filled with bone matter and placed in the disc space between the two vertebrae to increase the likelihood of fusion. Bones may be realigned depending on how much one vertebra has slipped forward on the other. The most important steps are restoring stability and making sure the nerves have no pressure on them.