Sarcoma
advertisement

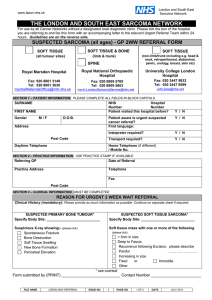
SARCOMA SUSPECTED CANCER REFERRAL FORM Date of GP decision to refer: Click here to enter a date. No. of pages sent: ESSEX AND BEDS & HERTS: London Sarcoma Service ask for direct referral – NO ULTRASOUND DELAY ANGLIA: Addenbrookes and Norfolk & Norwich run a diagnostic service, triaging patients to Birmingham. It is recommended that GPs refer to the tertiary centre (WITHIN 48 HOURS) following results of X-ray. NOTE: Do not refer HIV-associated Kaposi’s sarcoma with this form. PATIENT DETAILS –Must provide current telephone number. Last name: Gender: M ☐ F ☐ NHS No: Address: First name: DOB: Telephone (Day): Telephone (Evening): Mobile No.: Patient agrees to telephone message being left? Y ☐ N ☐ Transport required? Y ☐ Email: Interpreter required? Y ☐ Language/Hearing: Learning difficulties? Y ☐ Mental capacity assessment required? Y ☐ Known safeguarding concerns? Y ☐ Mobility requirements (unable climb on/off bed)? Y☐ SYMPTOMS & CLINICAL EXAMINATIONS STOP: If suspected bone metastases from an unknown primary, refer using local cancer of the unknown primary form X-ray suggests the possibility of bone sarcoma [2015] ☐ ☐ Spontaneous fracture ☐ Bone destruction ☐ Soft tissue swelling ☐ New bone formation ☐ Periosteal elevation ☐ Unexplained bone swelling or pain [2015] SOFT TISSUE SARCOMA ☐ Ultrasound suggests soft tissue sarcoma [2015] if available ☐ Ultrasound uncertain, but clinical concern [2015] if available Mass with 1 or more of the following: ☐ >5cm in size ☐ Deep to fascia ☐ Painful ☐ Fixed ☐ Increasing in size [2015] Please provide more details, if the following: ☐ Other ☐ Recurrence following excision IF <25 years, call consultant and refer urgently (WITHIN 48 HOURS) [2015]. Complete and send this form so patient is tracked. Please attach a Patient Summary including: ☐ Referral letter (if applicable) ☐ Investigation results GP DETAILS GP name: Practice Code: Address: TEL: FAX: Practice email: INVESTIGATIONS IN SUPPORT OF REFERRAL You don’t need to wait for results of tests to refer. ☐ BONE: X-ray ☐ SOFT TISSUE: Ultrasound (if available) Please attach reports with completed referral form. Location: Size: PATIENT MEDICAL HISTORY (MANDATORY) Existing conditions & Risk factors (inc smoking status): Current medication: Y☐ Y☐ Y☐ Y☐ Allergies Anticoagulants/Antiplatelets Immunosuppressants Diabetic WHO Patient Performance status (see key below) ☐0 ☐1 ☐2 ☐3 ☐4 DISCUSSIONS WITH PATIENT PRIOR TO REFERRAL Cancer needs to be excluded Patient given referral information leaflet Date(s) unavailable next 14 days: ☐ PMH ☐ Up-to date medications list and indications If your patient does not meet NICE suspected cancer referral criteria, but you feel they warrant further investigation, please disclose full details in your referral letter. 0 1 2 3 4 WHO PATIENT PERFORMANCE STATUS KEY Fully active, able to carry on all pre-disease performance without restriction Restricted in physically strenuous activity but ambulatory and able to carry out light/sedentary work, e.g. house or office work. Ambulatory and capable of self-care, but unable to carry out work activities. Up and active > 50% of waking hours. Capable of only limited self-care. Confined to bed or chair >50% of waking hours. Completely disabled. Cannot carry out any self-care. Totally confined to bed or chair. FOR GUIDANCE ON SYMPTOMS & HOSPITAL CONTACT DETAILS, SEE REVERSE OF THIS FORM. ☐ ☐ < 25 YEARS X-ray suggests possibility of bone sarcoma [2015] QUERY ≥ 25 YEARS Unexplained bone swelling or pain Unexplained lump that is increasing in size [2015] Unexplained lump that is increasing in size [2015] Unexplained bone swelling or pain V. urgent direct access X-ray in 48hrs (primary care must ensure result is acted on) Urgent direct access ultrasound in 2 wks (primary care must ensure result is acted on) IF AVAILABLE Urgent direct access ultrasound in 2 wks (primary care must ensure result is acted on) IF AVAILABLE V. urgent direct access X-ray in 48hrs (primary care must ensure result is acted on) X-ray suggests possibility of bone sarcoma [2015] QUERY Ultrasound suggests soft tissue sarcoma or clinical concern persists [2015] IF AVAILABLE CALL CENTRE: REFER WITHIN 48 HOURS SUSPECTED CANCER REFERRAL WITHIN 14 DAYS **There is a separate referral form for patients aged <16 years** ANGLIA Diagnostic services (triage to Birmingham) Addenbrookes Use e-referral (Choose & Book) Add-tr.nhsoutpatientreferrals@nhs.net Tel: 01223 216214 ESSEX and BEDS & HERTS SOFT TISSUE (ALL SITES) Royal Marsden Hospital FAX: 020 8661 3149 TEL: 020 8661 3630 CentralReferralsOffice@rmh.nhs.uk SOFT TISSUE (Non-limb/trunk, i.e. head & neck, pelvic, skin, breast, retroperitoneal, urology, abdominal, etc. University College London Hospital FAX: 020 3447 9932 TEL: 020 3447 9599 ucl-tr.LondonSarcomaService@nhs.net Norfolk & Norwich Use e-referral (Choose & Book) FAX: 01603 286876 SOFT TISSUE SARCOMA (Limb & Trunk) Royal National Orthopaedic Hospital FAX: 020 8909 5709 TEL: 020 8909 5603 mo-tr.LondonSarcomaService@nhs.net BONE SARCOMA Royal National Orthopaedic Hospital FAX: 020 8909 5709 TEL: 020 8909 5603 mo-tr.LondonSarcomaService@nhs.net