Supplementary Information Supplementary Table 1 Summary of end
advertisement

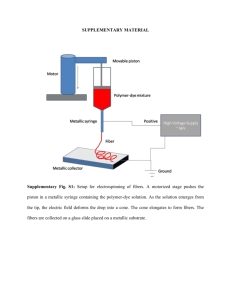
Supplementary Information Supplementary Table 1 Summary of end target feedback and scoring “On-time” “Too slow” “Too fast” End target display Patients & normal controls ≤ 800 ms ≤ 800 ms > 800 ms Not Not Shown Shown > 800 ms target entry time Duration-matched ≥ 500 ms and ≥ 500 ms and controls target entry > 800 ms > 800 ms < 500 ms < 500 ms No Yes No Yes No 1 0 0 0 0 ≤ 800 ms ≤ 800 ms Hold in target? Yes Points 2 time Target entry time was measured as the time between leaving the start circle and entering the end circle (Fig. 1C). “Hold in target?” = “Yes” for trials where the fingertip cursor remained within the end circle for 1500 ms after entering it. S1 Supplementary Figure 1 Block diagrams of two different computational models of reaching control. The top diagram is the same as Figure 4 with a dashed box highlighting the portion of the model that differs between the inverse model-based command generator (described in the main text) and the forward model-based command generator. In the forward model scheme, the desired trajectory is compared to the output of the forward model and this difference is multiplied by a feedforward gain, which results in the motor command. S2 Supplementary Figure 2 Comparison of fit results. (A) The desired trajectory duration (dur) was lower for normal controls compared to patients and duration-matched controls (both P < 0.05). (B) The feedback position gain (KP) was significantly lower for patients than either control group (both P < 0.0001). (C-D) There were no significant differences feedback velocity gain (Kv) and feedback delay (Δ). S3 Supplementary Figure 3 Patient dysmetria is not systematically affected by damping changes. Modifying arm damping in a way that might improve dysmetria did not cause patients to behave more like controls with regard to both dysmetria (A,C) and early velocity (B,D). *P < 0.05. S4 Supplementary Figure 4 Simulating characteristics of ataxia under different conditions. Model parameters used to match the behavior of the example hypermetric patient shown in Fig. 5A (Experimental) were modified to examine other possible conditions. (A) By increasing inertia of the plant (+i 50% = 50% increase; +i 100% = 100% increase), the model predicted an increase in hypermetria that has been previously reported (Manto et al., 1994). (B) Altering the duration of the desired trajectory (+dur 50% = 50% increase; -dur 50% = 50% decrease) produced changes in hypermetria as seen in movements with different timing constraints (Topka et al., 1998). (C) Increasing the feedback gains to match average control subject values (Kp = 6.8, Kv = 1.6) predicted more oscillations near the end target (intention tremor). S5 Supplementary Figure 5 Simulation of behavioral variability. (A) Same behavior of hypermetric patient shown in Figure 2B. (B-F) Simulations of null reaching when variability is added to a given parameter from trial to trial (iIM = internal model inertia value, Kp = position feedback gain, Kv = velocity feedback gain, dur = desired trajectory duration, Δ = feedback delay). Adding variability to the internal model inertia value (B) most closely resembles the observed behavior, suggesting that internal model variability may account for much of the variance in observed behavior. S6 Supplementary Table 2 Summary of acceleration and deceleration values Group Peak Accelerations (°/s2) Null +i -i +b -b All Controls 496.4 ± 130.7 387.8 ± 107.4 587.9 ± 131.4 396.4 ± 114.1 554.7 ± 124.8 Duration-matched controls 398.0 ± 118.9 304.5 ± 89.7 499.8 ± 125.1 309.0 ± 111.8 474.7 ± 136.3 All Patients 389.5 ± 125.3 296.0 ± 86.1 434.7 ± 108.9 332.2 ± 129.4 429.4 ± 121.6 Hypermetric Patients 287.6 ± 69.0 252.1 ± 58.8 360.4 ± 79.7 245.7 ± 52.8 352.4 ± 96.0 Hypometric Patients Peak Decelerations (°/s2) 485.1 ± 76.7 355.0 ± 98.4 525.4 ± 83.1 459.3 ± 102.5 521.9 ± 103.4 All Controls 419.7 ± 181.7 366.8 ± 95.1 615.8 ± 217.1 244.9 ± 56.5 750.9 ± 153.6 Duration-matched controls All Patients 271.4 ± 58.6 361.5 ± 124.6 309.0 ± 81.1 292.3 ± 87.2 487.1 ± 175.2 415.2 ± 167.0 198.9 ± 47.7 270.1 ± 107.1 697.4 ± 182.2 549.1 ± 160.0 Hypermetric Patients 320.4 ± 82.9 279.0 ± 101.0 351.6 ± 156.0 265.7 ± 142.1 504.5 ± 169.1 Hypometric Patients 340.8 ± 79.6 286.0 ± 77.9 416.6 ± 109.2 255.8 ± 71.3 581.0 ± 176.0 Acceleration Ratio (Peak Acc./Peak Dec.) All Controls 1.26 ± 0.28 1.06 ± 0.16 1.00 ± 0.20 1.61 ± 0.32 0.74 ± 0.12 Duration-matched controls 1.45 ± 0.22 0.99 ± 0.18 1.07 ± 0.26 1.54 ± 0.39 0.69 ± 0.15 All Patients 1.13 ± 0.41 1.10 ± 0.49 1.15 ± 0.38 1.40 ± 0.64 0.82 ± 0.28 Hypermetric Patients 0.92 ± 0.16 0.95 ± 0.21 1.11 ± 0.29 1.16 ± 0.61 0.71 ± 0.10 Hypometric Patients 1.49 ± 0.44 1.36 ± 0.70 1.34 ± 0.42 1.87 ± 0.44 0.98 ± 0.41 Average values ± standard deviation; Null, no perturbation; +i, increased inertia; -i, decreased inertia; +b, increased damping; -b, increased damping. S7 Supplementary Figure 6 Example of average position, velocity and acceleration profiles for the same control subject as Figure 2A. (A) The position profile was smooth and accurate. Thin arrow indicates time of peak acceleration and thick arrow indicates time of peak deceleration. (B) The velocity profile was bell-shaped. (C) The acceleration profile reveals some asymmetry, as the peak acceleration is larger than the peak deceleration. The raw acceleration data (orange, solid) was derived from position data recorded by the KINARM's sensors. The acceleration was smoothed using a forward-backward moving average (the acceleration value at each time point was averaged with the 4 nearest acceleration values) to reduce artifact introduced by differentiating data from position sensors. The moving average (black, dotted) was used for finding the peak acceleration and deceleration values. S8 Supplementary Figure 7 Results from the forward model-based command generator computational model. (A) Forward model-based model output of position traces for the typical control subject in Figure 3A is similar to inverse model-based model output (compare to Figure 3B) across different perturbation types. Thin arrows indicate time of peak acceleration and thick arrows indicate time of peak deceleration. (B) Forward model-based model output of dysmetria difference and S9 early velocity difference for the control group was similar to the behavior and inverse model-based model output of the control group shown in Figure 3C. Error bars indicate standard deviation. (C and D) Best forward model-based model fits (green dashed) for the same (C) hypermetric patient and (D) hypometric patient shown in Figure 2B, C are very similar to the inverse model-based model fits shown in Figure 5A, B. (E) As with the inverse model-based model, the forward model-based model inertia bias was highly correlated with dysmetria (R = 0.880, P = 0.001). Overshooting was best fit by forward model inertia values that were below the actual inertia of the arm (i.e. the actual arm was “heavier” than the internal model estimate). S10 SUPPLEMENTARY EXPERIMENTAL PROCEDURES Summary of scoring and end target display Immediately following each trial, subjects were provided with visual feedback on their speed and accuracy. The end target changed to: green for acceptable movements and blue for slow movements (target entry time > 800ms). The inside of the circle turned black when the cursor did not stay within the end target. For a subset of control subjects (referred to as “duration-matched controls”), the target turned red if the target entry time was less than 500 ms. The end target feedback and scoring system are summarized in Supplementary Table 1. The instructions were structured to prioritize timing over accuracy to discourage patients from making overtly slow feedback-guided movements that would mask dysmetria (Topka et al., 1998). Alternative computational models of reaching control In addition to the inverse model-based command generator computational model described in the main manuscript, we also simulated arm movements with a forward model-based command generator computational model (Supplementary Fig. 1). In this framework, the forward model-based controller requires the addition of a feedforward gain (KFF) in order to produce motor commands (Miall et al., 1993). It has been suggested that the inverse and forward modeling schemes can lead to very similar output if the parameters within the model are properly chosen (Miall et al., 1993). By comparing the model fits of the forward model-based controller and inverse-model based controller (compare: Supplementary Fig. 7A, B to Fig. 3B, C; Supplementary Fig. 7 C-E to Fig. 5A-C), it is clear that both models are capable of capturing the behavior examined in this study. In the main text we explore the inverse-model based controller in more detail, as it has fewer free parameters than the forward model version. It is worth noting that, although both models are sufficient to explain many of the observations in this study, models of similar architecture have been cast in doubt by previous researchers for multi-joint movements in force fields (Bhushan and Shadmehr, 1999) and two-dimensional manual tracking with delayed visual feedback (Miall and Jackson, 2006). A more general framework, such as optimal feedback control (Todorov and Jordan, 2002; Todorov, 2004), which also incorporates internal models, may better S11 explain the results of other studies involving more complex movements. Furthermore, researchers have suggested that internal model output may be combined with sensory information using a Kalman Filter (Wolpert et al., 1995; Todorov, 2004; Shadmehr and Krakauer, 2008) to provide optimal state estimation. However, we did not include this sophisticated component in our controller in order to keep the modeling simple and transparent. There were no significant differences between the parameter fits (root mean squared error (RMSE), position feedback gain (KP), velocity feedback gain (KV), and feedback delay (Δ); all P > 0.08 according to paired t-tests) for the two different models for the respective groups. In addition, similar to the modeling results of the inverse model-based controller, the forward model-based controller led to significantly lower KP values among patients (average = 2.5 Nm/rad) as compared to controls (average = 6.4 Nm/rad; P < 0.001), but no differences in RMSE, (KV), or (Δ) (all P > 0.06 according to t-tests). Lastly, the KFF were not significantly different between the groups (P = 0.23). SUPPLEMENTARY RESULTS Damping does not systematically improve patient movement We studied patients moving with increased or decreased plant damping. This was done to determine if the benefits that we saw during Experiment 3 were specific to altering inertia or if other dynamic compensations also improved movement. Our simulations suggested that the damping that would improve the dysmetria would produce an undesirable change in the early velocity. For example, increased damping (+b) for hypermetric patients would reduce overshoot but further slow the movement. By comparing results shown in Fig. 6 and Supplementary Fig. 3, it appears that changing inertia systematically improves patient movements, whereas changing damping does not. Simulating known characteristics of cerebellar ataxia S12 We used our model to predict features of cerebellar ataxia that have been previously reported. We simulated an increase in patient overshoot as mass is added to a limb (Manto et al., 1994). We took the model parameters used for fitting the exemplary hypermetric patient (Fig. 5A), and increased the plant inertia (iPL) by 50 and 100%, while other parameters were unchanged (i.e. internal model estimates, feedback parameters, etc.). We were able to predict similar kinematics in that hypermetria increased with inertial load (Supplementary Fig. 4A). Our model predictions also matched the observation that hypermetria increases with movement speed (Topka et al., 1998) (Supplementary Fig. 4B). This occurs because faster movements involve larger accelerations and thus, misestimates of inertia would lead to larger errors before feedback corrections take place. Our model fits suggest that patients have lower position feedback gain as compared to controls (Supplementary Fig. 2B). The motor control systems for patients might employ reduced feedback gain in order to avoid instability caused by poor feedforward control (due to internal model biases and variability). This reduction in feedback gain agrees with methods for controlling systems with disturbances (Ioannou and Sun, 1995). We examined this idea by once again starting with the model parameters that provided the best fit for the average movement of the hypermetric patient. The feedback gains were increased to the average control subject values (Kp = 6.8, Kv = 1.6) while all other parameters were unchanged. Our model predicted greater oscillations near the endpoint (intention tremor) that appear to grow in magnitude and thus the system appears to be less stable (Supplementary Fig. 4C). Since patients are also highly variable, a large portion of movements would overshoot the target even more than the average movement shown. For such larger overshoots, the increased feedback gains would cause even greater oscillations than those shown here. Simulating variability To investigate the increased movement variability observed in cerebellar patients, we simulated dysmetric movements and added noise to various parameters (Supplementary Fig. 5). The parameters derived from the model fit shown in Figure 5A were used to generate the trajectory of the average movement. For a S13 given simulation set, a specific parameter (iPL, Kp, Kv, dur, Δ) was selected as the “variable parameter.” Seventy trials were simulated such that on each trial, the value of the variable parameter was selected from a normal distribution with mean equal to the parameter fit value and standard deviation (SD) specified as follows: the SD was chosen such that the ratio between the standard deviation and mean (coefficient of variation, CV) was equal to 0.7. This CV value was chosen for the simulations because it produced a range of dysmetria values comparable to the behavior. The simulation with iPL as the variable parameter (Supplementary Fig. 5B) most closely matched the behavior. Specifically, the iPL simulation was the only parameter that resulted in the particular endpoint error that we observed in this patient—predominantly overshooting with a few trials of undershooting. The iPL simulation also produced a good match for the oscillations at the end of the movement— they are small and quickly converge to the end target, even for large overshoots. Thus, these simulations support the idea that internal model variability alone can account for a large portion of movement variability and hence, patient internal models are probably both variable and biased. Examination of acceleration and deceleration We computed the peak acceleration, peak deceleration, and the ratio between the two values (termed acceleration ratio) for the different subject groups and different conditions (Supplementary Table 2). Similar to a previously mentioned study involving hypermetric wrist movements (Manto et al., 1994), we found that hypermetric patients had a lower average acceleration ratio than controls. We also found that hypometric patients had the highest average acceleration ratio of all the groups. In contrast to some previous studies involving targeted single joint movements (Hogan, 1984; Manto et al., 1994; Richardson and Flash, 2002), the acceleration ratio for controls was > 1, indicating some asymmetry in the velocity profile. This could be because the interplay between task demands (i.e. accuracy and timing requirements) and signal-dependent noise (Harris and Wolpert, 1998) was different from the previously mentioned studies. The deviation from symmetric velocity profiles may explain some of the discrepancies between our model predictions and the actual data, since, to reduce complexity, our model assumes symmetric velocity profiles. In addition, a close inspection of the acceleration ratios reveals that control subject perturbations do not perfectly match patient movements in the S14 null condition. For example, the reduced inertia (-i) perturbation for controls (which we argue is similar to hypometric patients moving in the null condition) led to a reduction in the acceleration ratio while hypometric patients in the null condition had the largest acceleration ratios. The aforementioned differences in feedback gains (Supplementary Figs. 2B and 4C) might account for this discrepancy. Further investigation employing expanded models, detailed analysis of kinematics, and inspection of EMG during the movement will likely yield additional subtle, yet important, characteristics of patient movement. Example of velocity and acceleration curves Although we focused on position profiles in this study, the velocity and acceleration profiles may also provide insight regarding abnormalities of patient movement. The position, velocity and acceleration profiles for the same control subject shown in Figure 2A are displayed in Supplementary Figure 6. The average acceleration was smoothed by computing the forward-backward moving average (5 points, equally weighted) to avoid noise created by numerical approximations of the second derivative of position data recorded by the robot sensors. Supplementary References Bhushan N, Shadmehr R. Computational nature of human adaptive control during learning of reaching movements in force fields. Biol Cybern 1999; 81: 39–60. Harris CM, Wolpert DM. Signal-dependent noise determines motor planning. Nature 1998; 394: 780–784. Hogan N. An organizing principle for a class of voluntary movements. J. Neurosci. 1984; 4: 2745–2754. Ioannou PA, Sun J. Robust Adaptive Control. Har/Dis. Prentice Hall PTR; 1995. Manto M, Godaux E, Jacquy J. Cerebellar hypermetria is larger when the inertial load is artificially increased. Ann. Neurol. 1994; 35: 45–52. Miall RC, Jackson JK. Adaptation to visual feedback delays in manual tracking: evidence against the Smith Predictor model of human visually guided action. Exp Brain Res 2006; 172: 77–84. Miall RC, Weir DJ, Wolpert DM, Stein JF. Is the cerebellum a smith predictor? J Mot Behav 1993; 25: 203– 216. Richardson MJE, Flash T. Comparing smooth arm movements with the two-thirds power law and the related segmented-control hypothesis. J. Neurosci. 2002; 22: 8201–8211. S15 Shadmehr R, Krakauer JW. A computational neuroanatomy for motor control. Experimental Brain Research 2008; 185: 359–381. Todorov E, Jordan MI. Optimal feedback control as a theory of motor coordination. Nat. Neurosci. 2002; 5: 1226–1235. Todorov E. Optimality principles in sensorimotor control. Nature Neuroscience 2004; 7: 907–915. Topka H, Konczak J, Dichgans J. Coordination of multi-joint arm movements in cerebellar ataxia: Exp. Brain Res. 1998; 119: 483–492. Wolpert DM, Ghahramani Z, Jordan MI. An internal model for sensorimotor integration. Science 1995; 269: 1880–1882. S16