review of systems questionnaire
advertisement

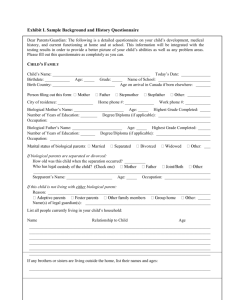
North Springs Psychiatry LLC Amanda J. Batterbee, PMHNP-BC 1880 Office Club Pointe Suite #1200 Colorado Springs, Colorado 80920 Phone: (719) 272-8222 Fax: (719) 272-8223 Patient Questionnaire REVIEW OF SYSTEMS QUESTIONNAIRE Patient Name: Date: __________________ What do you most want to discuss today? __________________________________________ Please circle GENERAL Fatigue Decreased appetite Fevers Weight loss Weight gain Insomnia Do you have a living will Do you smoke Do you drink alcohol Are you in pain 1-10 EYES, EARS, NOSE and THROAT Visual changes Hearing loss Sore throat Nasal Congestion Yes Runny nose Ear Pain NECK Swollen Glands Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes RESPIRATORY Shortness of breath Cough Wheezing Yes Yes Yes CARDIOVASCULAR Chest pain Palpitations High blood pressure Stroke Yes Yes Yes Yes DIABETES A1C Results Blood Sugars CGM – Sensor Problems CGM – Sensor Readings Digestion problems Labs Lipids Loss of consciousness Medications Meter Problems Meter Readings Pump Problems Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes ROS QUESTIONNAIRE WITH VITALS 01/27/2011 Pump Settings Yes Sores on feet Yes Tingling/numbness –Feet Yes GASTROINTESTINAL Abdominal pain Constipation Bloody stool Diarrhea Heartburn Nausea/Vomiting Yes GENITOURINARY Change in bowel habits Painful urination Yes Bloody urine Increased urination Leaking Urine Erectile Dysfunction Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes GYNECOLOGIC Irregular Menses Abn. Vaginal Discharge Pelvic Pain Pain with intercourse Painful Menses Pregnant Yes SKIN Rashes Itching Mole Changes Yes Yes Yes Yes Yes Yes Yes Yes MUSCULOSKELETAL Joint pain Yes Where? Muscle pain Yes Where? Leg swelling Yes Where? NEUROLOGIC Headaches Dizziness Difficulty walking Numbness or tingling Yes Yes Yes Yes PSYCHIATRIC Anxiety Yes Irritability Yes Sexual Problems Yes Suicidal Ideation Yes Depression Yes Concerns about your Yes emotional or physical safety? ROS QUESTIONNAIRE WITH VITALS 01/27/2011 ROS QUESTIONNAIRE WITH VITALS 01/27/2011