View Word DOC
advertisement

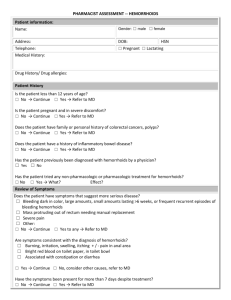
PHARMACIST ASSESSMENT – DYSMENORRHEA Patient Name: HSN: Address: DOB: Telephone: ☐ Lactating Medical History ☐ Liver dysfunction ☐ Renal dysfunction (CrCl ) Drug History/ Drug allergies: Patient History History of gynecological disorders other than typical dysmenorrhea symptoms (ex: endometriosis, ovarian cysts, fibroids), inflammatory bowel disease, or irritable bowel syndrome? ☐ Yes Refer to MD History of IUD insertion within last six months? ☐ No Continue ☐ Yes Refer to MD Is the patient trying to conceive or possibly pregnant? ☐ No Continue ☐ Yes Refer to MD At what age did the symptoms first appear? ☐ 6 months - 1 year after menarche up to age 25 → Continue ☐ Onset immediately at menarch, after age 25, or after at least 2 years of painless periods → Refer to MD (possible pelvic abnormality) Previously diagnosed with dysmenorrhea by a physician? ☐ Yes ☐ No Does the patient have a history of, or risk factors for, cardiovascular or cerebrovascular disease? (see full guidelines for definitions of risk factors and CVD) ☐ No Continue ☐ Yes Prefer treatment options other than NSAIDs (particularly avoid diclofenac and celecoxib). Refer to MD if NSAID deemed necessary. Has any pharmacologic or non-pharmacologic treatment been used for symptoms? ☐ No ☐ Yes What was tried? What was the effect? Review of Symptoms Pain accompanied by a fever? ☐ No → Continue ☐ Yes → Refer to MD (possible infection) Any rectal pain or bleeding ? ☐ No → Continue ☐ Yes → Refer to MD Atypical gynaecological symptoms present? (pain during sexual intercourse, excessive bleeding during menstrual period, intermenstrual bleeding, post-coital bleeding, vaginal discharge) ☐ No → Continue ☐ Yes → Refer to MD Pain occurs in ovulatory cycles? ☐ Yes → Continue ☐ No → Refer to MD (pain onset premenstrually or lasting throughout the cycle often found with endometriosis) Symptoms consistent with the diagnosis of dysmenorrhea? ☐ cramps in lower abdomen, pelvis ☐ accompanied by other symptoms of prostaglandin excess (nausea, vomiting, diarrhea, backache, thigh pain, headache, dizziness) ☐ pain starts shortly before onset of menstruation ☐ Yes → Proceed to treatment ☐ No → Consider other conditions / refer to MD Treatment ☐ Non-pharmacologic treatment recommended: ☐ OTC medication recommended: ☐ Prescribe three day supply of prescription strength NSAID X three months. Options include: ☐ Ibuprofen: 600 to 800 mg three times daily when required. Maximum 3200 mg /day. ☐ Mefenamic acid: 500mg initially at onset of bleeding and symptoms, followed by 250mg every 6 hours for 3-5 days ☐ Naproxen base: 500mg initially, followed by 250mg every 6 to 8 hours, when required. Maximum 1.25g/day ☐ Other NSAID: (loading dose followed by usual recommended dose for 3-5 days) Prescription Issued for minor ailment Rationale for prescribing: Rx: (Name, strength) Quantity (may prescribe quantity for 3-5 days of treatment and up to three cycles, plus one refill): Dosage Directions: pseudoDIN: 00951095 Counseling ☐ Instructions on non-pharmacologic measures ☐ Expect relief of symptoms within 30 to 60 minutes; if no response after 3 cycles or symptoms worsen, contact your pharmacist or MD Follow-up scheduled in 2 to 3 days (date): ☐ In pharmacy ☐ Telephone (number: ) ☐ Symptoms resolved – advise continuing therapy as needed monthly. Contact MD for authorization of refills past initial 3 months or refer patient to MD ☐ Symptoms improved but still bothersome --> Continue treatment for 3 months; if still a concern, consider trial of a different NSAID (MAXIMUM two trials) or refer patient to MD. ☐ No effect or symptoms worsening --> Refer to MD Prescribing Pharmacist: Name: Pharmacy: Tel: Signature: Fax: Email: Date: