Tuberculin Certification (e3799)
advertisement
")
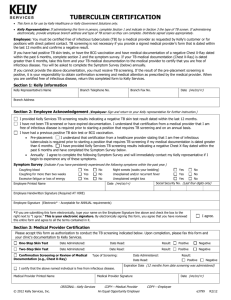
TUBERCULIN CERTIFICATION Kelly Representative: If administering this form in person, complete Section 1 and indicate in Section 3 the type of TB screen. If administering electronically, provide candidate/employee branch address and type of TB screen so they can complete. Distribute signed copies appropriately. TB screening is an annual requirement; refer to Tuberculosis Screening Guidelines (e3800) for instructions. Candidate/Employee: You must be certified free of infectious tuberculosis (TB) by a medical provider as requested by Kelly’s customer or for positions with direct patient contact. TB screening is not necessary if you provide a signed medical provider’s form that is dated within the last 12 months and confirms a negative result. If you have had positive TB skin tests, or have the BCG vaccination and have medical documentation of a negative Chest X-Ray dated within the past 6 months, complete section 2 and the symptom survey. If your TB medical documentation (Chest X-Ray) is dated greater than 6 months, take this form and your TB medical documentation to the medical provider to certify that you are free of infectious disease. You will be asked to complete the Symptom Survey (below) annually. If you cannot provide the above documentation, you must receive TB screening. If the result of the pre-placement screening is positive, it is your responsibility to obtain confirmation screening and medical attention as prescribed by the medical provider. When you are certified free of infectious disease, return this completed form to Kelly Services. Kelly will pay for the cost of any annually required TB screenings and you may be compensated for your time to complete such screening at minimum wage. Section 1: Kelly Information Kelly Representative’s Name Branch Telephone No. Date (MM/DD/YY) Branch Fax No. Branch Address Section 2: Acknowledgement (Candidate/Employee: Sign and return to your Kelly representative for further instruction.) I provided Kelly Services TB screening results indicating a negative TB skin test result dated within the last 12 months. I have not been TB screened or have expired documentation. I understand that certification from a medical provider that I am free of infectious disease is required prior to starting a position that requires TB screening and on an annual basis. I have had a previous positive TB skin test or BCG vaccination. Pre-placement: I understand that certification from a healthcare provider stating that I am free of infectious tuberculosis is required prior to starting a position that requires TB screening if my medical documentation is dated greater than 6 months. I have provided Kelly Services TB screening results indicating a negative Chest X-Ray dated within the past 6 months and have completed the Symptom Survey below. Annually: I agree to complete the following Symptom Survey and will immediately contact my Kelly representative if I begin to experience any of these symptoms. Symptom Survey (Indicate if you have persistently experienced the following symptoms within the past year.) Coughing blood Coughing for more than two weeks Excessive fatigue or loss of energy Yes Yes Yes No No No Night sweats (soaks your bedding) Unexplained and/or recurrent fever Unexplained weight loss No No No Social Security No. (Last four digits only) Date (MM/DD/YY) Printed Name Yes Yes Yes Handwritten Signature (Required AT HIRE) Signature (Electronic* - Acceptable for ANNUAL requirements) *If you are submitting this form electronically, type your name on the Signature line above and check the box to the right next to “I agree.” This is your electronic signature. By electronically signing this form, you agree that you have reviewed this entire form and agree to all the terms contained in it. I agree. Section 3: Medical Provider Certification Please accept this form as authorization to conduct the TB screening indicated below. Upon completion, please fax this form and your clinic’s documentation to Kelly Services at 1-877-397-9207. One-Step Skin Test Date Administered: Date Read: Result: Positive Negative Two-Step Skin Test Date Administered: Date Read: Result: Positive Negative Confirmation Screening or Review of Medical Documentation (e.g., Chest X-Ray) Type of Screening: Date Read: I certify that the above named individual is free from infectious disease. Medical Provider Printed Name ORIGINALKelly Services © 2014 Kelly Services, Inc. Date Administered: Result: Positive Negative Expiration Date (12 mos. from date screening administered): Date (MM/DD/YY) Medical Provider Signature COPYMedical Provider COPYCandidate/Employee An Equal Opportunity Employer e3799 R10/14