Script (DOC) - RHD Australia
advertisement
 - RHD Australia")
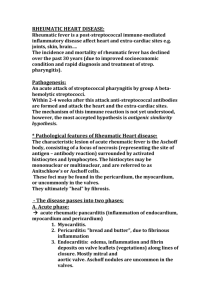
Secondary Prevention – Script SLIDE 1 Welcome to Rheumatic Heart Disease Australia’s Health Provider Education Series; educational resources for clinicians by clinicians. RHD Australia is an initiative of Menzies School of Health Research, James Cook University and Baker IDI, and is supported by the Commonwealth Department of Health and Ageing. This presentation is about the secondary prevention of acute rheumatic fever and rheumatic heart disease, and the challenges presented in delivering secondary antibiotic prophylaxis, especially in rural and remote settings. SLIDE 2 This presentation was developed by Malcolm McDonald, who is based in Cairns in Queensland and Keith Edwards, from Darwin in the Northern Territory. Both specialists have a longstanding interest in acute rheumatic fever and rheumatic heart disease, and remote health care delivery SLIDE 3 The learning objectives of this module cover the principles of secondary prevention, the tools used for delivering secondary prevention, the role of register-based programs, the role of primary health care and the practical challenges of delivering secondary prevention programs. SLIDE 4 The take home messages of this module are: That secondary prevention is difficult, complicated and expensive. Yet it is still the most cost effective approach we have, at least at present. The greatest challenges in service delivery come from communities suffering the highest risk of acute rheumatic fever and rheumatic heart disease, especially those in remote regions of northern Australia. These communities bear one of the highset disease burdens for ARF and RHD in the world. Effective prevention requires national evidence-based guidelines, regional and national rheumatic heart disease and acute rheumatic fever registers, and high quality recall systems based in primary health care. Education is essential. Ongoing education must be directed at health professionals, patients and their families. The primary aim of secondary prophylaxis is to prevent ‘at risk’ days. Don’t be late, and never miss a jab. SLIDE 5 For further information, you can consult the Australian Guideline for prevention, diagnosis and management of acute rheumatic fever and rheumatic heart disease, which can be found at the RHD Australia website. The 2012 guidelines have been substantially revised and updated. SLIDE 6 There is also a quick reference guide that provides a helpful summary for day-to-day clinical practice SLIDE 7 More information about other areas of prevention, diagnosis and management of acute rheumatic fever and rheumatic heart disease can be found at the RHD Australia website in the health provider education series. These resources will be regularly updated and revised. SLIDE 8 All the recommendations in this education module are consistent with those of the Therapeutic Guidelines - Antibiotic, and the address of the Therapeutic Guideline website is provided should you require further information. SLIDE 9 We should remind you that this educational series uses a number of abbreviations, and they include using ARF for acute rheumatic fever and RHD for rheumatic heart disease, GAS for group A beta-haemolytic streptococcus (the bacteria which indirectly causes ARF), and BPG for benzathine penicillin G (the most effective antibiotic for preventing recurrent ARF and progressive RHD) . SLIDE 10 Before going any further, we will cover the principles of secondary prevention. Secondary prevention first requires the diagnosis of acute rheumatic fever and/or rheumatic heart disease. Once the diagnosis has been made, the person must be given long term antimicrobial or antibiotic prophylaxis to prevent recurrent episodes of acute rheumatic fever, and associated valve inflammation which can progress to rheumatic heart disease. Successful delivery of antimicrobial prophylaxis requires a register based secondary prevention program, effective recall systems, and a functioning primary health care service. SLIDE 11 The disease process that leads to acute rheumatic fever and rheumatic heart disease is quite complicated and often poorly understood. However, it seems that between 5 and 7% of the population has a genetically determined predisposition to ARF. The process usually begins in early childhood, with children between the ages of 5 and 14 being most at risk. ARF is a disease of childhood disadvantage, and particularly occurs in populations and households where there is poverty, over-crowding and a poor standard of, or access to household hygiene facilities. In this setting, children are at high risk of infectious diseases, especially group A streptococcal infection. Over the first few years of life, children in these setting often have recurrent group A streptococcal infection, certainly of the skin and probably of the throat. Each GAS infection provokes an immune response. In some children, repeated infection provokes an escalating response; and this is sometimes called immune priming. Once a threshold or tipping point has been reached, the child has an exaggerated and specific immune response that precipitates the first episode of ARF. Fortunately, the frequency of Group A streptococcal infection tends to diminish over time. Nevertheless, it’s the recurrences of ARF that cause cumulative inflammation and valve damage that ultimately results in rheumatic heart disease. SLIDE 12 There are several points along the pathway where we can intervene with prevention measures. Primordial and primary prevention are covered in another module, and this can be found on the RHDAustralia website in the Health provider education series. Today we’re looking at secondary prevention. That is, giving intramuscular benzathine penicillin G on a regular basis over a prolonged period of time in order to prevent recurrent ARF and cumulative heart valve damage; that is rheumatic heart disease. Of course, what we want to avoid, if possible, is the tertiary management of rheumatic heart disease; that includes the management of heart failure, heart valve replacement and all the associated complications. Tertiary management is required if the diagnosis is delayed, and not made until late in the disease process. Tertiary management of RHD carries a high cost, both financial and personal, for people with RHD, their families, the whole community and the health system on every level. This is in marked contrast to the relative cost-effectiveness of providing secondary prevention. SLIDE 13 The peak incidence of acute rheumatic fever in communities with the highest rates of disease is between the ages of 5 and 14. The peak prevalence of rheumatic heart disease is later, in the early 20’s. So the critical period for secondary prevention is in this early period, before the development of rheumatic heart disease. Thus secondary prevention is aimed at preventing debilitating disease in adolescents and young adults during the most productive and fertile years of their lives. SLIDE 14 Fortunately, the Group A streptococcus remains exquisitely sensitive to penicillin. Let’s hope it remains so. Benzathine penicillin G (otherwise known as BPG) is a long-acting penicillin, and we know that the antibiotic levels in the blood are sufficient to prevent GAS infection for about three weeks. Protective levels drop off quickly during the 4th week. This is one reason why it is so important to never miss a scheduled BPG injection SLIDE 15 This slide outlines the recommended options for secondary prevention. Many children and adolescents will not tolerate a painful injection every 3 weeks, so the best compromise is to give a benzathine penicillin injection every 4 weeks. Three weekly injections may still be required for specific high risk groups. The recommended regimen for giving benzathine penicillin G is outlined in the chart here. This can also be found in the Australian Guidelines for Prevention, Diagnosis and Management of acute rheumatic fever and rheumatic heart disease located on the RHD Australia website. [Please leave time for the chart to be read] SLIDE 16 There are specific settings where we should consider giving 3 weekly benzathine penicillin injections, even though it may not be well received. These are: moderate or severe rheumatic carditis, where there is a history of valve surgery, or when there has been a previously confirmed breakthrough of acute rheumatic fever, despite good adherence to four weekly injections. SLIDE 17 For the majority of children and adolescents, we use a four weekly regimen, and we regard day 28 as the last day that the benzathine penicillin can be given. Every day after day 28 is called an ‘at risk day’ for acute rheumatic fever recurrence. This is where we can target our service delivery, which must be proactive and opportunistic. We must aim to give the injections between days 21 to 28. After each injection, the recall date should be reset to day 28 Remember, it is always safer to give BPG early rather than late. SLIDE 18 There are many thorny issues and curly questions related to delivery of secondary prevention. Very little research has been done into the practicalities of giving secondary prevention at the primary health care level, which means that most of the recommendations are not evidence based. Most people receiving secondary prevention are asymptomatic children, adolescents, and young adults. Benzathine penicillin G injections really hurt, and giving them successfully requires a good deal of experience and skill. Unfortunately, many clinics in remote Aboriginal communities where rates of disease are highest also have highest turnover of clinic staff. Whether the program succeeds at a primary care level largely depends on the individual priorities of senior staff in these clinics, and their enthusiasm for delivery of adequate secondary prevention. Some health providers in remote clinical settings do not understand that each person on the ARF prevention program must receive ALL of their injections on time to actually prevent the recurrence of acute rheumatic fever. Unfortunately, because clinics are often overburdened with conflicting demands, there may be long waiting times. If people are left to wait too long whilst contemplating a painful injection in the backside, they may be tempted to leave the clinic. So it’s really important that each clinic has a fast track system to make sure that people requiring secondary prevention are seen in a timely manner, and that doses are not missed. SLIDE 19 There are other issues in remote Aboriginal communities that are often not considered. For example, it is often important to have female nurses or aboriginal health workers giving the injections to young women. It is just as important for male health workers and male nurses to give the injections to boys and young men. There is also potential for family kinship conflicts, whereby clinic staff or patients may encounter ‘poison cousins’ or other culturally confronting situations with family members when people front up for BPG injections. In addition, clinics are often pressed for resources that are needed for family support and education regarding the ARF/RHD prevention program. It can be difficult to provide an education service, when so many conflicting and often more urgent demands present themselves. Another issue is the site of delivery of the injections. Injections may be given in a clinic, in the home, at the school or elsewhere. If they are only given in the clinic then transport may be a problem. This particularly applies to people who live in remote outstations, who may have no access to a vehicle, or indeed money for fuel. Mobility is another issue. Families and communities are often highly mobile and adolescents sent away to boarding school, or spend time living with other families. So it is both important and challenging to ensure continuity of service delivery. Arrangements should be made in advance for kids to get their injections at boarding school, in other communities they visit, or when they have family trips to town. This requires good communication between primary health centres and with the central ARF/RHD register. Good communication is key to delivering effective secondary prevention. Health professionals need to ask about family plans for travel and provide people on the ARF prevention program, or parents in the case of children, with copies of their relevant reports and/or correspondence to take with them. They should also call and FAX ahead the material to the health service or school taking over responsibility for secondary prevention delivery. The success of a secondary prevention program also depends on the frequency of specialist visits. This includes paediatricians, physicians, cardiologists, dentists, allied health staff and echocardiographers. The provision of specialist services to remote and rural communities is infrequent at best, and non-existent at worst. If a specialist appointment is missed by someone on the secondary prevention program, it may be several months before another appointment can be made. This hiatus can put a child or young adult at risk of a potentially severe adverse outcome. Lastly, there have been occasions when supply of benzathine penicillin has been irregular and interrupted. Obviously this can have a major impact on the delivery of a secondary prevention program. SLIDE 20 When giving the injections, it’s important to ensure that we use a twenty-one gauge needle. Using a smaller gauge needle can actually increase the pain. Ensure that the syringe is warmed when taken out of the refrigerator, at least to room temperature. A cold injection hurts much more. Always give the injection in the upper outer quadrant of the buttock and, prior to inserting the needle, apply firm pressure with the thumb at the injection site for at least ten seconds beforehand. This seems to reduce the pain. SLIDE 21 If using an alcohol swab, make sure that the alcohol has dried before giving the injection. Give the injection slowly, over two to three minutes, and try to provide distraction, with conversation and especially with young children and adolescents. Some people add a small amount of lignocaine to the injection, but this is currently not recommended with the preloaded syringes that we use in Australia. SLIDE 22 This table outlines the duration of secondary antibiotic prophylaxis. This depends on the timing of the last episode of ARF and the severity of the rheumatic heart disease. People with a history of acute rheumatic fever and no rheumatic heart disease, or mild rheumatic heart disease, should have a minimum of 10 years prophylaxis after the last episode of acute rheumatic fever, or until they are 21 years of age, whichever is longer. People with moderate rheumatic heart disease should have antibiotic prophylaxis at least until the age of 35 years. People with severe rheumatic heart disease, and those who have had cardiac surgery, may need to continue with prophylaxis until after 40 years of age, and sometimes for life. More detailed information about the duration of secondary prophylaxis can be found in the appropriate section of the National Guidelines, which can be found on the RHDAustralia website. SLIDE 23 So, despite our best efforts, in Australia only 20% of people on rheumatic heart disease prevention programs receive 80% of their required benzathine penicillin G injections. In addition, we know that 30% of acute rheumatic fever episodes are recurrences. These occur when people have missed injections; even one injection. Despite our efforts, we’re not getting it completely right. That is why we must emphasise that one late or missed injection puts that person at risk of recurrent acute rhematic fever. Everyone, that is the clinical staff, the patient, family and community, needs to understand the key message, and that message is; “Don’t be late. Never miss a jab.” SLIDE 24 We’re now going to look at the 3 requirements for a successful register-based acute rheumatic fever and rheumatic heart disease prevention program. The first is to ensure successful provision of secondary prophylaxis by updating, generating and distributing community lists of people with known acute rheumatic fever and rheumatic heart disease. With this information, the primary health service can target service delivery with accuracy The program must be able to identify any gaps in service delivery and feed that information back to the primary care services. This ensures that resources are appropriately targeted and local solutions are developed for local problems. SLIDE 25 The second is to facilitate co-ordination of service delivery by: recording details of people who require follow up, generating regular reports to enable timely recall and review, ensuring that people with acute rheumatic fever and rheumatic heart disease are not lost to follow up, and facilitating appropriate education for clinic staff, people with rheumatic fever and rheumatic heart disease, their families and the broader community. Community understanding and support are essential to ensuring that improvements in delivery of secondary prevention are sustainable. SLIDE 26 The third requirement is the collection and use of epidemiological data. We collect data to monitor the incidence of acute rheumatic fever and the prevalence of rheumatic heart disease in each region. These data are also used: for program evaluation, to identify research needs and prioritise resources. SLIDE 27 At this point, we should go through the Ten Commandments for successful delivery of secondary prevention. The first is thou shalt mobilise and marshal political commitment, at all levels, so that there is sustainable funding of infrastructure to support delivery of the ARF/RHD prevention program, nationally and regionally. The second commandment is thou shalt ensure that the ARF/RHD prevention program has a backbone advisory committee that follows and promotes evidenced-based care. The third is thou shalt ensure that there is an up-to-date and accurate electronic data base, or register, of people diagnosed with ARF and RHD The fourth: thou shalt integrate the program with the public health system and with primary health care delivery. The fifth: thou shalt ensure the ability to find new cases and accurately diagnose acute rheumatic heart fever and rheumatic heart disease. SLIDE 28 The sixth commandment: thou shalt make acute rheumatic fever and rheumatic heart disease are notifiable diseases The seventh: thou shalt monitor service delivery. The eighth: thou shalt provide culturally appropriate and ongoing education to patients, families, communities and health care providers. The ninth: thou shalt establish a priority system for those at the highest risk. And the tenth commandment: thou shall ensure that there is an independent evaluation system built into the program. SLIDE 29 Register based secondary prevention programs for acute rheumatic fever and rheumatic heart disease face several challenges and these seem to be universal around the globe. The first is that the populations at highest risk also tend to be highly mobile. This can frustrate patient recall systems, service delivery and proper documentation. The second problem is that we have issues with both under-diagnosis and over-diagnosis of acute rheumatic fever and rheumatic heart disease. Under-diagnosis means that some kids with ARF/RHD miss out on secondary prophylaxis. Progressive RHD could have been prevented but that opportunity was lost. Over-diagnosis can mean that a healthy kid can be unnecessarily subjected to painful 4-weekly injection over many years for absolutely no benefit. The third is under-reporting by health professionals of identified disease. A missed case is a missed opportunity to prevent a potentially debilitating, and life-threatening, disease. The fourth problem we face concerns the legal difficulties with informed consent and local privacy legislation. These issues can seriously interfere with the functions of a disease register. Lastly, wherever we go, we know that people with acute rheumatic fever and rheumatic heart disease are the most disadvantaged and politically disenfranchised people in any country. They rarely have a voice. This is why advocacy so important. All health providers have a responsibility to advocate for properly-resourced disease prevention programs – including a rheumatic heart disease prevention program. SLIDE 31 Let’s recap the main points covered, and the take home messages from this presentation. Secondary prevention is both complicated and expensive. The program is difficult to deliver and BPG injections are really painful. Nevertheless, this is the most cost-effective approach we have at the moment. Secondary prevention provides great challenges in service delivery, especially in the populations at highest risk. Successful delivery requires evidence-based guidelines, an accurate and up-to-date rheumatic heart disease and rheumatic fever register, functional, high quality recall systems and service delivery that is based in primary care. It also requires a functional primary care system. A successful secondary prevention program must provide ongoing education to health professionals, patients, families and the community at large. The major message is that we must prevent any ‘at risk days’. ‘Don’t be late. Never miss a jab.’ SLIDE 32 This is to remind you that all of the information contained in this module can be found in the Australian Guideline for the Prevention, Diagnosis and Management of acute rheumatic fever and rheumatic heart disease. This guideline is available on the RHD Australia website. SLIDE 33 There is also a quick reference guide that provides particularly useful summaries for clinical practice. SLIDE 34 And you can find more information on the prevention, diagnosis and management of ARF and RHD in other modules in the health provider education series, located on the RHDAustralia website. SLIDE 35 You can download these PowerPoint presentations and obtain additional resources at the same site by registering with the Health provider education series on the RHD Australia website. You’re also invited to ‘like us’ on our Facebook page to ensure you receive notifications regarding new or updated education modules. SLIDE 36 Finally, we invite you to test your knowledge about this subject with a brief self-assessment quiz.