Background Paper - Department of Social Services

Stakeholder Consultation Meeting –
Severe Behaviour Response Teams
Background Paper
Introduction
The Government convened the inaugural Ministerial Dementia Forum on 11 September 2014. One of the key goals of this Forum was to seek feedback on alternate mechanisms for addressing the needs of aged care residents experiencing severe and extreme Behavioural and Psychological Symptoms of Dementia
(BPSD) .
People experiencing very severe and extreme BPSD can have continual or episodic behaviours which are extremely challenging for other residents and very difficult for care staff of aged care homes to manage.
A lack of specialised support was identified as a significant problem by most Forum participants. Providers noted that they often have challenges in accessing support for people with severe BPSD and/or had challenges in implementing strategies to support people with severe BPSD. The use of teams of health professionals to complement the Dementia Behaviour Management Advisory Service (DBMAS) in supporting aged care homes to provide appropriate care was one of the options subsequently recommended to Government by the Dementia Forum Working Group.
DBMAS is funded by the Australian Government to provide advice and assistance to home care providers, residential aged care providers and hospitals caring for people with dementia. They provide clinical interventions to help aged care staff, health professionals and family carers improve their care of people with dementia where the behaviour of the person with dementia impacts on their care. DBMAS functions include assessment and short term case management, clinical supervision, mentoring and modelling of behaviour management techniques and provision of education and tailored information workshops. In
2013-14 DBMAS had provided a total of 6,715 episodes of service, of which 3,020 (45 per cent) were referrals from aged care homes.
On 4 February 2015, the Government announced that Severe Behaviour Response Teams (SBRT) would be established to assist residential aged care homes who request assistance with residents experiencing the most severe BPSD.
SBRTs will be specialised teams of healthcare professionals able to visit residents exhibiting very severe and extreme BPSD, assess the causes, and assist care staff in residential aged care homes to address and deal with these behaviours. They will act as a top tier to DBMAS, focusing solely on people experiencing very severe and extreme BPSD in residential aged care.
The first phase of the SBRTs will commence nationally later this year, following a competitive tender process. Following the Analysis of Dementia Programmes, a second phase will see the SBRTs integrated with DBMAS from 2016-17 as the current DBMAS funding agreements conclude in June 2016.
Funding
The Commonwealth will invest $54.5 million over four years to establish SBRTs.
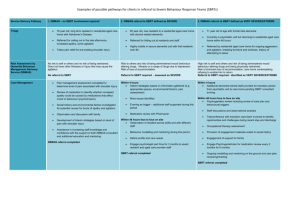
Table 1 below outlines the estimated $113.6 million of funding which will be provided to the SBRT and
DBMAS programmes in the four years from 2015-16, noting that the services of DBMAS are also available to home and acute care clients.
PO Box 7576 Canberra Business Centre ACT 2610
Email Facsimile Telephone 1300 653 227
National Relay Service: TTY: 133 677, Speak and listen: 1300 555 727, Internet relay: www.relayservice.com.au
Year
SBRT
DBMAS
*Estimate
Table 1 – SBRT & DBMAS Funding 2015-16 to 2018-19
2015-16 2016-17 2017-18 2018-19
$12.7m $13.2m $13.9m 14.7m
$14.4m $14.6m* $14.9m* $15.2m*
TOTAL
$54.5m
$59.1m*
Timing
A competitive tender process for Phase One of the SBRTs is expected to open during April 2015, with the service to commence in July/August 2015. This will be for a national SBRT operation, although bids for individual state or territory SBRTs will be considered. Tenders from either single service providers or consortiums of service providers will be considered.
This will be followed by a competitive tender process in late 2015 for an initial 3 or 4 year contract for the
Phase 2 integrated SBRT/DBMAS.
Formal evaluation mechanisms will be a requirement of both the Phase One and Phase Two contracts.
SBRT Framework
The Government will set the broad parameters for the SBRT, while allowing tenderers to propose their own specific operating model.
Target Clientele
SBRTs will focus on residents of all Commonwealth funded residential aged care services, including flexibly funded services and Multi-Purpose Services. Home care clients are out of scope. SBRTs will, however, be able to assist clients who were admitted to acute care from Commonwealth funded residential aged care and who are in the process of returning to residential aged care. Clients in an aged care home on a respite basis will also be eligible.
SBRTs will focus solely on aged care residents posing a significant risk to either themselves or others.
These are likely to be residents who align to the high end of Tier 5 or Tier 6 of the BPSD Seven-Tiered
Model of Service Delivery 1 . Table 2 outlines the number of aged care residents expected to need assistance from SBRTs, based on the assumption that around one per cent will experience severe and extreme BPSD.
Table 2 – Estimate of Residents with Severe and Extreme BPSD
Year 2015-16 2016-17 2017-18
Residents 2,426 2,489 2,574
Note: Figures based on Department of Social Services projections of aged care resident numbers.
2018-19
2,674
1
Brodaty, H., Draper, B., Low, L-F. Behavioural and psychological symptoms of dementia – a 7- tiered triangular model of service delivery.
Medical Journal of Australia, 2003;178(5):231-234.
2
Referral
Referrals will be made to SBRTs via DBMAS. As is currently the case, referrals can be made to DBMAS by residential aged care providers or family members with guardianship. If DBMAS considers the issue falls within the clientele scope outlined above, rather than one of their staff, the DBMAS will pass the referral to the SBRT.
This approach will make use of current infrastructure, ensure that teams from DBMAS and SBRTs are not both being called to address the same issue, and provide an inbuilt mechanism to facilitate coordination between the two services.
There will be no Aged Care Assessment Team involvement in the referral process.
Service Scope
SBRTs will have a number of clear goals, specifically:
identify the causes/triggers of the severe and extreme behaviours being experienced by the resident;
assist care staff to resolve the immediate crisis and/or assist in alternative arrangements;
advise care staff on how to address episodic factors or environmental issues that may be triggering or exacerbating the resident’s behaviour;
advise care staff on dealing with longer term underlying causes of a resident’s behaviour;
assist staff in developing an immediate and longer term care plan for the resident;
liaise with general practitioners or other relevant health professionals regarding long term care of the resident;
provide follow up support and assistance;
hands on up-skilling and training of staff;
if needed request that DBMAS provide the aged care home with appropriate training;
minimise inappropriate resident referrals to acute care; and
assist aged care homes to reintegrate residents with severe behaviours returning from acute care.
If a resident is displaying behaviours beyond the management of a residential aged care facility the SBRT may consider referral to an appropriate setting like another specialised residential facility or a specific psychogeriatric unit.
SBRTs will respond to aged care homes within 24-48 hours.
The exact make up of a team responding to a specific referral will be decided by the SBRT and be determined by the nature of the issue(s) needing to be addressed.
3
DISCUSSION
On 18 March 2015 the Government is holding a consultation with stakeholders to seek feedback on the
SBRT Framework outlined in this paper. Specifically how it can be refined and improved. Discussions on alternate policy settings are not within the scope of this consultation.
Clientele and Referral
Overview
SBRTs will focus solely on aged care residents posing a significant risk to either themselves or others.
These are likely to be residents who align to the high end of Tier 5 or Tier 6 of the BPSD Seven-Tiered
Model of Service Delivery. Referrals will be made to SBRTs via DBMAS.
Framing Questions
Given that DBMAS will be making referrals based on information provided by the aged care home, is there a need for inclusion and exclusion criteria or a checklist to be developed to assist in this process?
1.
Multidisciplinary Teams
Overview
Very severe and extreme BPSD can manifest itself in a complex range of cognitive, physical, social, and emotional problems.
Due to the complexity and variability of very severe and extreme BPSD, a one size fits all approach is not appropriate.
A multidisciplinary team of specialists can use a collaborative approach to tackle issues from multiple angles, ensuring that care options are complementary and integrated, and not limited by any one health professional’s area of expertise.
SBRTs are intended to provide a direct line of access to multidisciplinary expertise for management of people with very severe and extreme BPSD.
The exact make up of a team responding to a specific referral will be decided by the SBRT and determined by the nature of the issue needing to be addressed.
Framing Questions
What is the scope of the specialist support that will be required?
Should the initial response be by a clinician, with at minimum registered nurse or clinical psychologist qualifications, who is then able to access further advice and hands-on assistance from appropriate medical experts such as geriatricians, psychogeriatricians, GPs, psychiatrists, pharmacists, nurse practitioners, and allied health professionals?
What role will the SBRT play in the long term care of the residents? Should they refer back to the DBMAS after the initial crisis is resolved or should they have an ongoing role?
4
2.
SBRT Use of Telehealth
Overview
Telehealth is an expanding sector of healthcare involving the use of telecommunication tools such as videoconferencing, skype and so on. A wide range of techniques fall into this sector, including the administrative, preventative, consultative and curative aspects of health care.
A GP treating a patient in a residential aged care home can refer the patient to a specialist for a video consultation. The specialist and the patient will be able to see and hear each other via video conferencing technology. Similarly both the GP and Specialist can be present during a supported telehealth consultation.
Telehealth has been shown to be a useful format for increasing accessibility to health services in regional, rural and remote areas, and when a situation needs more immediate intervention, it can allow for quicker access to specialist knowledge.
In relation to dementia care, the Victorian Government Cognitive Dementia and Memory Service programme has had some success with using telehealth as a medium for consultations.
2
It is not however the intention that telehealth would replace face to face consultation as a general rule.
Framing Questions
In the context of SBRTs, is telehealth appropriate for conducting preliminary consultation and assessment?
What type of assessments could be undertaken by telehealth?
Could this medium be used as a general first point of contact or should it be only used for rural and remote?
3.
Acute Care Transition
Overview
There is evidence to suggest that people with dementia being admitted to acute care for emergency treatment (81%) rather than elective treatment (19%) are more likely to experience a decline in health as a result of the hospital admission 3 .
When the person with dementia is exhibiting very severe and extreme BPSD then this is likely to be exacerbated.
Framing Questions
Is there value in the SBRT devising transition strategies both in the move from residential care to acute care, and from acute care to residential care?
4.
Other Issues
Framing Questions
What key performance indicators would be useful in assessing the performance of the SBRT programme?
Are there other issues we need to address?
2
Telehealth outreach to rural regions in a cognitive dementia and memory service (cdams) Dr Olivia Gobbo, Elizabeth Mullaly, Beth
Kirkwood. CDAMS - Caulfield Hospital, Alfred Health, Melbourne Victoria.
3
Grand, J. H., Caspar, S., & MacDonald, S. W. (2011). Clinical features and multidisciplinary approaches to dementia care. Journal of
Multidisciplinary Healthcare , 4 , 125 –147. doi:10.2147/JMDH.S17773
5