William C Smith paper 2014
advertisement

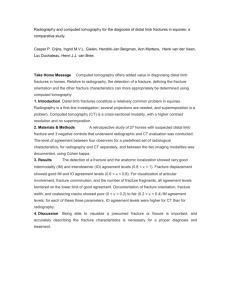
Senior Seminar Paper Cornell University College of Veterinary Medicine April 26, 2014 Femoral Fracture Repair in a Three Day Old Holstein Heifer Calf William Christopher Smith Clinical Advisor: Dr. Wade Walker Basic Science Advisors: Dr. Alan Nixon and Dr. Norman Ducharme 2 Abstract The patient, a three day old Holstein heifer calf was presented to Cornell’s Farm Animal hospital on April 6, 2014 for evaluation and treatment of a large swelling over the left hip as noticed by the owner. Radiographic evidence showed a complete, transverse, comminuted, mid-diaphyseal femoral fracture that had proximo-medial displacement. The calf was placed under general anesthesia and the comminution was stabilized using Cerclage wire. The fracture was stabilized in a two plate method placed at 90 degrees to one another; a tibial buttress plate was used to stabilize the fracture in the frontal plane and a limited contact/dynamic compression plate was used to stabilize the fracture in the sagittal plane. 6.5mm cancellous screws were used in the soft metaphyseal bone and 5.5mm cortical screws were used to engage both cortices of the femoral diaphysis and for compression of the dynamic compression plates. This paper discusses the different methods of fracture repair, selection of the appropriate orthopedic implant based on the nature of the fracture, and the inherent difficulties in repairing such fractures. 3 Introduction The idea of femoral fracture repair has been performed since veterinary surgery began, however most calves that have fractured femurs are unfortunately euthanized due to the nature of the complications that arise from the fracture itself or from the complications that could arise from the malunion of the femoral fragments. This calf was a genomex calf and it had been reported that the dam and the granddam were the most genetically valuable Holsteins in the country. The udder scores of the dam were very impressive at a 94 out of 100 and her offspring all had comparable scores. Cost of the open long bone fracture repair is typically the single most limiting factor in whether or not to attempt surgery. Due to the genetic value of this calf, the owner elected to have the femur repaired. Signalment and Case History A three day old Holstein heifer calf presented to the Cornell University Farm Animal Hospital on April 6, 2014, with a one day history of the owner noticing that the calf was unable to stand or bear weight on the left hindlimb. A large swelling was also noticed on the left hip. The owner presumed that the calf had been stepped on by her dam and causing a traumatic injury that prevented the calf from standing. Prior to the injury, the owner noted an uneventful parturition and that the calf had adequate colostrum intake. 4 Presentation and Diagnostics On presentation, the calf was bright, alert and responsive. Mucous membranes were pink and capillary refill time was less than two seconds. The calf had a temperature of 101.7 F, pulse rate of 150 bpm, and a respiratory rate of 120 bpm. A complete blood count and chemistry were performed and the results were unremarkable. Medio-lateral and cranio-caudal radiographs were then performed of the left hip and femoral area. The radiographs were performed in the large animal hospital and determined that the calf had sustained a complete, closed, transverse, mid-diaphyseal fracture with proximo-medial displacement of the distal fragment (Figure 1). The owner was informed of the radiographic findings and decided to proceed with repair and stabilization of the fracture. The following day, the calf was anesthetized preoperative radiographs were taken in the small animal hospital with a bucky and revealed that the distal fragment had a cranial comminution (Figure 2), which would need to be stabilized before the fracture could be plated or stabilized with an intramedullary nail or pin. If the comminution had not been recognized on radiographs, the distal fragment may have splintered upon securing the plate to the femur with cortical screws. The comminution would need stabilization with Cerclage wire before the plates could be secured to the femur. Problem List and Differentials On April 6, 2014, the patients problem list included the following: non-weight bearing lameness, swollen left thigh and tachypnea. The most common differentials according to the problems on initial presentation and signalment were a Salter Harris 5 Type 2 fracture and Diaphyseal fracture of the femur as well as a Coxofemoral luxation. Based on the radiographs in Figure 1 and Figure 2, the diagnosis was made of a complete, closed, transverse, comminuted, mid-diaphyseal femoral fracture with proximo-medial displacement. Surgical Treatment The owner decided to proceed with surgical intervention and have the fracture stabilized using two plates and Cerclage wire to stabilize the surperficial commminution. A venous catheter was placed and intravenous fluids were administered. The patient was premedicated and placed under general anesthesia and nerve blocks were performed, in order to ensure appropriate multi-modal analgesic management. The nerve blocks were aimed at the sciatic and femoral nerves and a combination of Bupivicaine and Dexmedetomidine was injected perineurally. These nerve blocks would serve two fold in blocking the motor function to the nerve for at least ten hours, whereas the sensory blockade would last almost twenty hours. The calf was then positioned in right lateral recumbency and the left hindlimb was wrapped with sterile vetwrap and the greater trochanter of the femur as well as the stifle was draped into the surgical site. The surgical site was aseptically prepared and sterile draping was applied. An approximately 20cm incision was made through the skin and subcutaneous tissues. The boundary between the gluteobiceps and vastus lateralis muscle was incised and retracted away from the lateral aspect of the femur. The distal fragment was located and the surperficial comminution was stabilized using a Cerclage wire, which was wrapped circumferentially around the distal fragment over top the comminution and 6 secured. The fracture was reduced and a thirteen hole tibial buttress plate was used on the lateral aspect of the femur, stabilizing the fracture in the frontal plane. Two 5.5mm cortical screws were placed in compression and 6.5mm cancellous screws were used in the soft metaphyseal and with cortical screws in neutral position in the diaphyseal bone. After adequate tightening of the screws, a second limited contact/dynamic compression plate was placed on the cranial aspect of the femur so that sagittal and rotation stabilization was achieved. A stent was placed over the incision to relieve tension and keep the incision site clean. Post-operative analgesics were not administered immediately following surgery due to the motor and sensory blockade achieved by the femoral and sciatic blocks. Following surgery, the left hind limb was cold-packed immediately and wrapped. Three days post-operation, a series of passive range of motion exercises were performed by placing the patients left hind limb in extension, flexion, and rotation every six hours. Outcome and Prognosis Twelve hours after surgery, the calf was noted to be able to stand and bear full weight on the left hind limb. The passive range of motion exercises were tolerated well by the calf and she was noted to have been moving around her ICU stall and able to lay down and rise without pain or discomfort. A slight fever was noted and two doses of Flunixin Meglumine were administered 24 hours apart. The fever resolved and no other complications were noted for the rest of the calf’s stay at the hospital. 7 Two weeks postoperatively radiographs were taken revealing bone callous over the fracture site and stable implants. There was no radiographic evidence of infection or loose screws (Figure 3). The prognosis for this calf is good due to the fact that the fracture seemed stable and callus was being produced (Figure 4). The literature dictates that prognosis and success rate of these fractures after the use of only one plate or an intramedullary pin or nail is guarded due to implant failure because of rotational forces exerted upon the fracture site that inevitably causes the implant to fail. With this type of repair, the fracture can become severely comminuted and the animal must be euthanized due to inability of the animal to stand or bear weight (5). According to one case report of twelve calves treated for femoral fractures, At necropsy, 42 days after surgery, the femurs with intramedullary pins were healing with slight malalignment and overriding. The femurs with half-pin assemblies were considered nonunions, with severe overriding, malalignment, and osteomyelitis; the femurs with bone plates and screws were healing, although the screws had loosened and allowed overriding with rotational malalignment of the fractures(6). Discussion Femoral fractures continue to present a problem and challenge to practicing veterinarians especially when it occurs in large animals. The inherent complications involved in such surgeries to correct these fractures continue to be a complicating factor despite the most rigorous attempts to control it(1). Femoral fractures are a very common source of fracture in dairy calves, due to the high incidence of manual 8 intervention during a dystocia. Many calves do not survive being pulled during a dystocia or have lasting effects due to it. In femoral fractures, the most common is a Salter Harris Type 2, through being pulled, however this calf was not part of a dystocia(3). Any coaptation to try and correct this fracture without surgery or the use of pins or plates would have predisposed the calf to instability and ultimately euthanasia. The fracture needed to be stabilized in two different planes, since there was no obliquity to help stabilize in any plane. If the fracture had an oblique fracture component, then the use of an intramedullary nail or pin would have been possible. Intramedullary pins and nails only provide axial stabilization of the fracture so that callous may form and the fracture is bridged by woven bone, however there is no rotational stabilization. The use of plates is needed when the fracture site is transverse and needs rotational stabilization(6). A fracture that needs rotational stabalization often needs to be plated in order to be successful. The disadvantages to plating a fracture are that the screws can become loose and there is a lot of hardware that can get infected or prevent angiogenesis. Two major complications associated with plating fractures are infection and implant breakdown(2). The advantages of plating a fracture are that rotational stabilization is provided and allows the fracture to be immobilized completely to help with bone healing. Another method of providing stabilization to the fracture site is the through the use of intramedullary pins or nails. These types of fracture stabilization are used in cases where support of the fracture site is achieved by placing pins through the medullary cavity after the two pieces are aligned. The disadvantages to using intramedullary nails or pins is that the rate of failure is high (6). The advantages are that the pins or nails are more cost effective and the application can be applied in a less traumatic fashion. 9 Conclusions Through the use of two bone plates and Cerclage wire, the two fragments of the femoral fracture were reduced and the comminution was secured. Femoral fracture in neonatal calves is of major concern to dairy producers worldwide due to the fact that these fractures cause loss of value to the producer. Surgery is the most viable option that I would recommend to producers of calves with these types of fractures. I would recommend to any dairy producer that the need for surgery for these calves is of utmost importance, no amount of external coaptation will allow this fracture to heal normally. Plating the fracture is the best option available for mid-diaphyseal transverse femoral fractures. 10 Figure 1: Day of presentation radiographs 11 Figure 2: Day of surgery radiographs, taken at the small animal clinic 12 Figure 3: Intra-Operative Radiographs 13 Figure 4: Two week post operation radiographs 14 References 1. Anderson, David. "Bovine Orthopedics, An Issue of Veterinary Clinics of North America: Food Animal Practice." Elsevier. N.p., Mar. 2014. Web. 14 Apr. 2014. 2. Andrews, A.H. "Bovine Medicine: Diseases and Husbandry of Cattle." Bovine Medicine. Jan. 2004. Web. 14 Apr. 2014. 3. Bellon, Jacques. "Use of a Novel Intramedullary Nail for Femoral Fracture Repair in Calves: 25 Cases (2008–2009)." AVMA. N.p., 1 June 2011. Web. 14 Apr. 2014. 4. Hoerdemann et al. “In-vitro comparison of LC-DCP- and LCP- constructs in the femur of newborn calves”. BMC Veterinary Research. June 2012. Web. 10 Apr. 2014 5. Ferguson, James G. “Fractures of the femur in newborn calves”. AVMA. N.p., Web. 5 Apr. 2014 6. Hance, S.R. “Study of 12 cases of femur fractures in calves less than two weeks old”. AABP Journal. Web. 5 Apr. 2014. 15 7. W. H. CRAWFORD. “Long Bone Fractures in Large Animals A Retrospective Study.” Journal of Veterinary Surgery. N.p. October 1985. Web. 6 Apr. 2014.