Applied Drug Therapy
advertisement

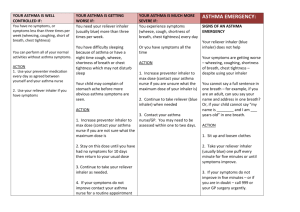
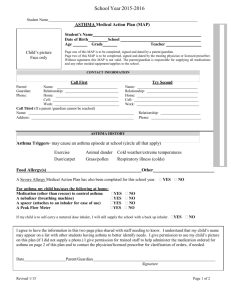
Advanced Pharmacology Asthma/COPD Homework 1 IMPORTANT! PLEASE READ! Before submitting this, please rename this file with your last name + first name initial + 2 Example: My name is Mike Oszko The name of this file should be: Oszkom2.doc Also, fill in the following information. Your homework will not be accepted without it! Name: Tracy Hill WU ID #: 20015608 _TH__ I hereby certify that the work submitted is my own, and that I have not plagiarized or violated any terms of the WU School of Nursing’s Classroom Integrity Policies. E-mail: tracy.hill@washburn.edu NOTE: You must insert your initials in the area of the line on the right Case AJ is a 22 year old male with a recent history of shortness of breath. You diagnose him with mild asthma, and decide to begin pharmacologic therapy. Using the prescription blank below, please write a prescription for what you believe to be the most appropriate STARTING medication to treat the ACUTE symptom (e.g., shortness of breath) for this patient (knowing, of course, that you can add or change medications later). (10 points) Primary Care Associates, Inc. 1020 Wellness Road Resume Speed, KS (913) 123-4567 Name AJ Date 2/24/2011 Address 1234 Maine St. City/State/Zip Lawrence, KS 66044 Age/Wt 22 / Rx Proventil HFA 90 mcg Disp: 1 (one) MDI Sig: Inh 2 puffs Q4-6 hours prn shortness of breath/wheezing [ Dispense as Written Refills none ] [ T. Hill, ARNP NOTE: This is a sample prescription form which is to be used for practice only. The contents hereon is not a valid prescription for any medication. Substitution Permitted DEA # ] 2. What education are you going to provide AJ regarding the prescription you just wrote? )Be concise! Use bullet points. Remember, you want AJ to remember what you’re telling him!) (10 points) Discuss role of medication - Albuterol is a beta-adrenergic agonist bronchodilator which means it is a smooth muscle relaxer/ reduces airway resistance (Edmunds & Mayhew, 2009, p. 192). It also produces a mild anti-inflammatory response. It is a “rescue medication” for patients with shortness of breath associated with asthma. Provide pt basic facts about asthma since this is a new diagnosis. Asthma exacerbation should be treated with SABA on an as needed basis on severity of symptoms. For shortness of breath and wheezing, dose should be 2 puffs every 4-6 hours as needed; up to 3 treatments can be used at 20 minute intervals for severe asthma attack. Inhaler can also be used 15-30 minutes before exercising to prevent symptoms while exercising. Use on an as needed basis and do not use if not needed. Discuss environmental control of asthma and triggers (smoking, dust, pet dander, allergens) and management of co-morbidities – discuss smoking cessation if pt or family smokes (airway clearance is impaired). Educate pt on signs of worsening and when to follow-up: increased cough, increased breathlessness, wheezing, especially at night; increased chest tightness. Assuming AJ has mild persistent or intermittent asthma (classify correctly) – re-evaluate frequently to determine correct severity. Develop a written action plan for correct severity of asthma. Discuss and test for Peak Expiratory Flow (PEF) and teach pt how to monitor lung function at home (Edmunds & Mayhew, 2009, p. 191). This will allow him to anticipate when breathing will become worse and to take the right medications or call provider before symptoms become too severe. Educate on most common side effects of albuterol – tachycardia, muscle tremors; Each canister provides 200 inhalations. It is recommended to prime the inhaler before using for the first time and in cases where the inhaler has not been used for more than 2 weeks by releasing four test sprays into the air, away from the face. There are about 200 metered doses in an inhaler. If you use up an inhaler in less than one month then we need to look at changing/adding medications and re-evaluating asthma control, therefore, there are no refills at this time on your inhaler. Please make a follow-up appointment for 1 month so we can evaluate your asthma, sooner if worsening. If AJ needs to use his inhaler more than every 4-6 hours, then he should call for follow-up appointment; pt needs to be re-evaluated in 1 month to determine how often albuterol has been used; if canister does not last entire month, pt probably using inhaler too often and is not well controlled, and needs to be re-evaluated for next step of asthma classification system and may need additional meds or adjustment in medications/ action plan. If a previously effective dose regimen fails to provide the usual response, this may be a marker of destabilization of asthma and requires reevaluation of the patient and the treatment regimen, giving special consideration to the possible need for anti-inflammatory treatment, such as corticosteroids (http://www.rxlist.com/proventil-drug.htm). Proper Inhaler Technique 1. Shake the inhaler vigorously. 2. Hold the inhaler about 2 fingers widths in front of your mouth 3. Exhale fully and completely through pursed lips. 4. Inhale slowly and deeply through an open mouth while pressing down on the canister 5. Close your mouth. Hold your breath for 5 to 10 seconds 6. Slowly breathe out through pursed lips. 7. Wait one minute to allow the medicine to work. 8. Repeat according to ordered puffs. 9. Rinse and gargle when finished to prevent hoarseness and infections in the mouth. 10. Cleanse the inhaler mouthpiece at least once daily by washing it with warm soapy water. 11. Rinse mouthpiece and dry well. (www.brynmawrhealth.org/thcn/files/ProperInhalerTechnique012008.pdf) Do you have any questions? 5 points: True or False (circle one) – Long-acting beta-2 agonists are more convenient than short-acting beta-2 agonists as rescue medications because they can be given only once or twice a day. The role of Beta2 agonists (SABA) is to provide relief of bronchospasm during exacerbation of asthma or pretreatment before exercise. Long acting beta agonist (LABA) should not be used as rescue meds (Edmunds & Mayhew, 2009, p. 192). The FDA recommends that LABA should not be used as first-line asthma agents; they should be added on only if other medications do not control asthma. LABA should not be used in place of a SABA to treat sudden wheezing. LABA may increase the chance that an asthma episode will be severe even though they decrease the frequency of asthma episodes (Edmunds & Mayhew, 2009, p. 199). References Edmunds, M. W., & Mayhew, M. S. (2009). Pharmacology for the Primary Care Provider (3rd ed.). St.Louis, MO: Mosby. Hamilton, R. J. (Ed.). (2011). Tarascon Pocket Pharmacopoeia: 2011 Classic Shirt-Pocket Edition (25th ed.). Sudbury, MA: Jones & Bartlett Learning, LLC. Turkoski, B. B., Lance, B. R., & Tomsik, E. A. (Eds.). (2010). Drug Information Handbook for Advanced Practice Nursing (11th ed.). Hudson, OH: Lexi-Comp.