Resident Aesthetic Clinics
advertisement

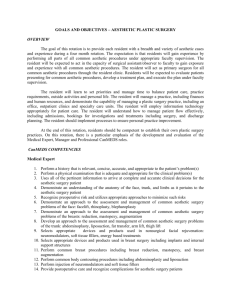
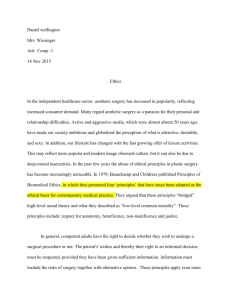
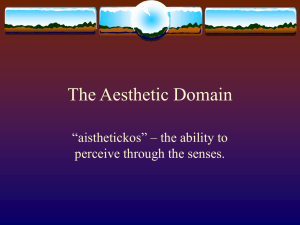
Identification of Best Practices for Resident Aesthetic Clinics in Plastic Surgery Training: The ACAPS National Survey C. Scott Hultman, MD, MBA, FACS;1 Cindy Wu, MD;1 Michael L. Bentz, MD;2 Richard J. Redett, MD;3 Bruce R. Shack, MD4; Lisa R. David, MD;5 Peter J. Taub,6 and Jeff E. Janis, MD7 From the Divisions and Departments of Plastic Surgery at University Of North Carolina, Chapel Hill, NC1 University of Wisconsin, Madison, WI2 Johns Hopkins University, Baltimore, MD3 Vanderbilt University, Nashville, TN4 Wake Forest University, Winston-Salem, NC5 Icahn School of Medicine at Mt. Sinai, New York, NY6 The Ohio State University, Columbus, OH7 Presented in part at the Annual Scientific Meeting of the American Society of Plastic Surgeons, San Diego, CA, October 2013; and the Annual Winter Retreat of the American Council of Academic Plastic Surgeons, Chicago, IL, December 2014 Funding: The UNC Ethel and James Valone Plastic Surgery Research Endowment Conflicts of Interest: no financial or commercial conflicts of interests Key Words: surgical education, aesthetic surgery Running Head: Best Practices for Resident Aesthetic Clinics Correspondence/Proofs/Inquiries/Reprints: C. Scott Hultman, MD, MBA, FACS Ethel and James Valone Distinguished Professor of Surgery Chief and Program Director, Division of Plastic Surgery Suite 7038, Burnett-Womack, CB#7195 University of North Carolina Chapel Hill, NC 27599-7195 Office: 919-966-2300; Fax: 919-966-3814 Email: cshult@med.unc.edu 2 ABSTRACT Introduction: Resident aesthetic clinics (RACs) have demonstrated good outcomes, reasonable patient satisfaction, and acceptable safety profiles, but few studies have evaluated their educational, financial, or medico-legal components. We sought to determine RAC best practices. Methods: We surveyed ACAPS Members (n=399), focusing on operational details, resident supervision, patient safety, medico-legal history, financial viability, and research opportunities. Of the 96 respondents, 63 reported having a RAC. 56% of plastic surgery residency Program Directors responded. Results: RACs averaged 243 patient encounters and 53.9 procedures annually, over a mean period of 19.6 years. Full-time faculty (73%) supervised chief residents (84%) in all aspects of care (65%). Of the 63 RACs, 71% of facilities were accredited, 40 had a licensed procedural suite, 28 had inclusion/exclusion criteria, and 31 used anesthesiologists. 17 had overnight capability. 17 had a life safety plan. No cases of malignant hyperthermia occurred, but there was one facility death reported. 16 RACs (25%) had been involved in a lawsuit. 33 respondents reported financial viability of the RACs (52%). Net revenue was transferred to both the residents’ educational fund (41%) and divisional/departmental overhead (37%). Quality measures included: case logs (78%), morbidity/mortality conference (62%), resident surveys (52%), and patient satisfaction scores (46%). 14/63 (22%) of respondents have presented or published research specific to RACs. 80/96 (83.3%) of those surveyed believed RACs enhanced education. Conclusion: RACs are an important component of plastic surgery education. Most clinics are financially viable, but carry high malpractice risk and consume significant resources. Best practices, to maximize patient safety and optimize resident education, include use of accredited procedural rooms and direct faculty supervision of all components of care. word count: 268 3 INTRODUCTION Many plastic surgery training programs include a resident aesthetic clinic, in which trainees have increased autonomy in decision-making and patients have improved access to aesthetic surgery, through reduced charges. While many studies have demonstrated good outcomes,1-6 reasonable patient satisfaction,7,8 and an acceptable safety profile,9,10 few reports have rigorously evaluated the operational, financial, and medico-legal components of these programs.11-13 Even though most plastic surgery educators recognize the value of having a resident aesthetic clinic, many different models for such a learning environment exist,14-18 and best practices for this teaching paradigm have not yet been defined. As the surgical trainee gains experience in aesthetic surgery, this learner must also become an autonomous practitioner, mastering key competencies of not only patient care and medical knowledge, but also systems-based practice, communications, practice-based learning, and professionalism. The resident aesthetic clinic, in which trainees evaluate patients, form an operative plan, execute the procedure, and provide follow-up care, represents an ideal setting for gaining increased independence, under the close observation of supervising faculty members. This paper attempts to move our educational framework “one step closer” to knowing the optimal learning experience in aesthetic surgery. We hypothesize that resident aesthetic clinics represent a valuable, unique paradigm for surgical education, provided that clinical results are acceptable, patient and provider satisfaction remains high, and patient safety is given highest priority. The authors 4 will describe the current status of resident aesthetic clinics in plastic surgery training and will provide best-practice guidelines to achieve superior outcomes. MATERIALS AND METHODS We conducted an anonymous, 41-question, internet-based survey of all members of the American Council of Academic Plastic Surgeons (n=399). Our questionnaire (designed by the first author and constructed by PRRI, Beverly, MA) focused on the following components: demographic information about the respondents, operational details of the clinic, resident training and supervision, patient safety, medico-legal history, financial considerations, and research opportunities. The questionnaire was sent to ACAPS members three times, from October through December 2012. Overall response rate for ACAPS members was 24% (n=96). Response rate for Program Directors was 56% (49 PDs from 87 institutions), representing over half of all training programs. Of the 96 respondents, 63 reported that their institution included a resident aesthetic clinic (66%). It should be noted that some institutions had more than one respondent. Thus, this survey reflects the opinions of ACAPS members who are involved with resident education, not specific programs. Using information obtained by this survey, and combining these data with their own experience, the authors developed a list of best practices for resident aesthetic clinics. These best practices were further refined, as a result of the discussion between panelists and attendees, at the 2013 ACAPS Annual Spring 5 Retreat, and further refined by the ACAPS Aesthetic Surgery Task Force at the 2014 Annual Winter retreat of ACAPS. RESULTS Demographics of Respondents. Overall response rate was 96 out of 399 ACAPS members, or 24%. Of the 96 respondents, 49 were program directors and 31 were chiefs or chairs of plastic surgery (Figure 1). Only 5 residency coordinators participated in the survey. Mean length of time in practice was 20 years, with a range of 0-40 years (Figure 2). Regarding type of practice, the vast majority of respondents had mostly reconstructive practices (n=76), compared to a minority of respondents who had mostly aesthetic practices (n=9) (Figure 3). In terms of the training programs, respondents reported the following mix of residency programs: integrated, n=35; independent, n=34; integrated and independent, n=27. The following organizational structure was reported for the plastic surgery practices: Division of Surgery at a Medical School, n=72; Department of a Medical School, n=19; Private Practice, n=5. Sixty-three out of 96 respondents, or 66%, reported the presence of a RAC, in which “plastic surgery residents had a focused cosmetic experience with some degree of autonomy.” Operational Details. RACs have been in practice for a mean of 19.6 years, with a range of 1-50 years (Figure 4). In terms of clinical volume, respondents reported a median of 88 patients and an average of 243 patients treated each year, with a range of 2-2000 encounters per year (Figure 5). When asked about procedures done at the RAC, respondents noted a median of 25 and an average of 6 53.9 procedures done each year, with a range of 0-300 cases per year (Figure 6). Components of the RACs, specific to location of patient encounters, include a combination of examination rooms and surgical suites (Figure 7), with 40 of the 63 clinics including access to a licensed operating room. Resident Supervision. Thirty-five out of 64 respondents (54%) who reported having a RAC indicated that Resident Aesthetic Clinic was a formal rotation in their residency program. Although respondents noted that chief residents represented the largest group of participants (n=53), lower level residents also have some degree of participation in the RAC (Figure 8). Nearly all residents (60 out of 64) provide continuity of care for their patients. According to the respondents, residents receive supervision mostly by full-time core faculty (Figure 9), who usually oversee all components of perioperative and intraoperative care (Figure 10). Patient Safety. Although the majority of RACs have some type of accreditation, 18 out of 63 respondents with RACS reported no accreditation (Figure 11). Furthermore, 28 out of 63 respondents with RACs reported a list of inclusion/exclusion criteria for cases, and only 17 respondents having a Life Safety Plan for the RAC. An anesthesiologist administers anesthesia in 31 out of 38 RACs with operative capability, whereas other personnel are used for this function in the remaining RACs (CRNA, 3; nursing staff, 2; surgeon, 2). Seventeen of the 35 clinics with operative capability reported the ability to recover patients overnight. Medico-legal History. Of the 64 respondents who indicated that their institution had a RAC, one ACAPS member reported a patient death in the facility, and two ACAPs members reported patient deaths within 30 days of the procedure. 7 Our cohort of ACAPS members observed no cases of malignant hyperthermia. Sixteen of the 62 ACAPS members (26%) indicated that their RAC has been involved in a lawsuit. Regarding malpractice insurance models, most groups are self-insured and pay premiums to a group trust (Figure 12). Three of the 63 respondents with RACs noted that patients must sign a waiver, releasing residents from malpractice liability or to limit award for damages. Financial Viability. Although 18 respondents did not know if their RACs were financially viable, 33 respondents indicated that their RACs were, compared to 13 respondents who reported that the RACs were not financially viable. The large majority of attending surgeons do not receive any financial remuneration, but some of the respondents do receive compensation from professional fees, teaching stipend, or a medial directorship. Almost all RACs offer discounted fees (59 out of 63, or 94%), and most RACs charge for the initial consultation (39 out of 63, or 62%). The most effective method for patient recruitment was listed as “word of mouth” (61 out of 63, or 97%). Faculty practices contribute various types of resources to the RACs, in addition to resident supervision (Figure 14), such as clinic space, scheduling, nursing support, and disposable supplies. If profitable, net income is primarily transferred to a residents’ education fund, but some of the gains are transferred back to the Division or Department, presumably to cover overhead costs (Figure 15). Only a small fraction of the positive net income is directed toward incentive plans for the faculty, to the Dean or the hospital, or toward an operating reserve. 8 Research and Outcomes Effectiveness. Respondents indicated that RACs use a number of different methodologies to measure the effectiveness of the educational experience, with review of resident case logs and morbidity and mortality conferences as the most popular techniques (Figure 16). Fourteen of the 64 respondents with RACs have presented related data at national scientific meetings, and 12 respondents have published their research in peer-reviewed, scientific journals. The overwhelming perception is that RACs have a positive effect on plastic surgery training (Figure 17). The majority of respondents were neutral when asked about the impact of the RAC on their practice (n=36), but only a minority of respondents reported that the RAC was a liability for the practice (n=7) (Figure 18). DISCUSSION Resident aesthetic clinics serve as an important component of graduate medical education in plastic surgery. Most clinics are financially viable but carry a high malpractice risk and consume considerable resources. Best practices, to maximize patient safety and optimize resident education, include use of accredited procedural rooms, having anesthesiologists provide anesthesia, and providing appropriate faculty supervision at all stages of patient care. The educational concept and implementation of Resident Aesthetic Clinics is not new, and has been implemented in various specialties including plastic surgery, otolaryngology,19 and dermatology.20 In fact, the literature is replete with manuscripts addressing the mechanics of administrating Plastic Surgery Resident 9 Aesthetic Clinics, their educational benefit, and analyses of outcomes data. According to Neaman in 2010, 71% of plastic surgery residencies had a cosmetic surgery clinic, with 44% of the respondents noted that 100% of the cases performed there were cosmetic in nature.3 In 2006, the University of Kentucky group noted that the resident cosmetic surgery clinic contributed 82% of the resident’s total aesthetic procedures. This was completed with a 3.1% reoperative complication rate and no medicolegal litigation.4 Pyle and colleagues at Wake Forest reported that not only do residents gain added experience as surgeon in a resident driven clinic, but that patients are able to receive cosmetic surgery that they might not otherwise be able to access. They had no major complications, but did report a minor complication rate of 8%, and a revision rate of 14.4%.10 Freiburg and associates at the University of Toronto examined a retrospective survey of 265 patients with a 49% response rate, where 93% of patients said they would recommend the clinic (after a slightly lower rate the first year), and 93% would undergo the same procedure again if required. The highest patient satisfaction was seen in augmentation mammoplasty (9.1/10.0) and blepharoplasty (9.0/10.0), while rhytidectomy and rhinoplasty were lower at 7.8/10.00 and 6.9/10.0, respectively.8 At Georgetown University, Baker and colleagues evaluated satisfaction with resident injected fillers using a FACE-Q survey. They demonstrated a 91% rate of being satisfied or very satisfied with this evolving less invasive and highly popular injection in ten patients.7 10 At the American Association of Plastic Surgeons meeting in 2012, a two-year retrospective review of patient care from 2009-2011 at the Johns Hopkins Resident Cosmetic Surgery Clinic was presented. Rad and colleagues noted complications rates consistent with the mainstream cosmetic surgery literature, breaking down the procedures by type and body location. Their study sample included 115 patients who underwent 132 primary body-contouring procedures, and 53 patients who underwent 84 facial aesthetic procedures.9 Based on the published literature, as well as the ACAPS national survey, it is clear that resident education in aesthetic surgery must be grounded in principles of informed consent, appropriate patient selection, patient safety, teamwork, and critical assessment of outcomes. Fortunately, qualitative and quantitative instruments have been recently developed to assess outcomes, in terms of patient satisfaction, as well as objective measures.21-23 Furthermore, surgical educators are focusing on how to teach trainees aesthetic surgery—and reporting these results— within the framework competency- and milestone-based graduate medical education.24-26 Additional efforts have been pursued to educate residents about the importance of strategic marketing, accounting and finance, economic forces of competition, the supply chain, and regulatory/legal considerations, in the context of office-based surgery and aesthetic services.27-31 The Aesthetic Surgery Task Force of the American Council of Academic Plastic Surgeons endorses the concept a properly supervised Resident Aesthetic Clinic, provided that the following guidelines are considered and followed, to the greatest extent possible, within training programs accredited by the ACGME: 11 1. The educational experience should maximize resident autonomy, appropriate to level of training, as permitted by ACGME guidelines a. Residents must obtain a complete history and physical examination, with preoperative evaluation to include patient photographs b. Residents must discuss case with attending regarding operative plan c. Attendings must be present for planning and execution of procedure d. Residents must be involved with postoperative management, including complications e. Residents must be available for 24-7 coverage, with adequate faculty backup 2. Longitudinal, complete continuity of care is critical; no post-rotation handoffs should occur 3. The RAC must have a medical director for the Resident Aesthetic Clinic 4. The RAC must establish screening processes to eliminate inappropriate patients, using such pre-defined parameters as BMI, smoking status, uncontrolled diabetes or hypertension 5. The RAC must establish operative criteria such as inclusion/exclusion lists, length of case 6. Surgery must performed in accredited facilities only 7. The RAC must have close faculty supervision in both the clinic and operating room, including presence at the key components of procedure 8. The faculty must establish goals, objectives, targets for residents, track outcomes, provide regular review, and offer timely feedback 12 9. Real-time evaluation of competencies and milestones must be performed 10. The program director should review of operative logs to ensure diversity of cases, surgeons, and locations 11. The RAC must combine a robust clinic and operative experience with strong educational modules focused on aesthetic surgery, including lectures, indications and outcomes conferences, and a journal club 12. The medical director should moderate a formal Resident Clinic Outcomes Conference for entire division/department 13. The division/department should reinvest net income back into the aesthetic curriculum/program 14. The RAC can consider reduced fees to stimulate demand, by decreasing professional fees and charging facility fees high enough to cover overhead 15. The RAC should involve residents with strategic marketing of the practice 16. The RAC should have a dedicated administrative assistant to help run the program 17. Although aesthetic education should begin early in the training program, the RAC should be limited to Chief or Senior residents in Plastic Surgery 18. The educational curriculum should phase in the complexity of the cases as the resident skill set grows (for example, the trainee could start with breast and body procedures, then move to facial procedures) 19. Trainee experience at the RAC should occur after more traditional aesthetic surgery rotations have been completed and should be considered separate and distinct from faculty practices 13 20. Residents should not be allowed to perform botox, fillers, peels in the RAC, which instead should be used as an operative experience, for surgical procedures 14 REFERENCES 1. Morrison CM, Rotemberg SC, Moreira-Gonzalez A, Zinz JE. A survey of cosmetic surgery training in plastic surgery programs in the United States. Plast Reconstr Surg 2008;122:1570-8. 2. Oni G, Ahmad J, Zins JE, Kenkel JM. Cosmetic surgery training in the plastic surgery residency programs in the United States: How have we progressed in the last three years? Aesth Surg J 2011;31:445-55. 3. Neaman KC, Hill BC, Ebner Ford RD. Plastic surgery chief resident clinics: The current state of affairs. Plast Reconstr Surg 2010;126:626-633. Discussion 634-635. 4. Pu LLQ, Thornton BP, Vasconez HC. The educational value of a resident aesthetic surgery clinic: A 10-year review. Aesthetic Surg J 2006;26:41-4. 5. May JW Jr. Aesthetic surgery 101: resident education in aesthetic surgery, the MGH experience. Ann Plast Surg. 2003 Jun;50(6):561-6. 6. Momeni A, Goerke SM, Bannasch H, Arkudas A, Stark GB. The quality of aesthetic surgery training in plastic surgery residency: A survey among residents in Germany. Ann Plast Surg 2013 Jun;70(6):704-8 7. Iorio ML, Stolle E, Brown BJ, Christian CB, Baker SB. Plastic surgery training: Evaluating patient satisfaction with facial fillers in a resident clinic. Aesth Plast Surg 2012;36:1361-6. 8. Freiberg A, Giguère D, Ross DC, Taylor JR, Bell T, Kerluke LD. Are patients satisfied with results from residents performing aesthetic surgery? Plast Reconstr Surg. 1997 Dec;100(7):1824-31; discussion 1832-3. 9. Rad A, Burretta KJ, Im J, Manson PN. The chief resident aesthetic surgery clinic: A safe alternative for patients. Abstract presented at he 91st Annual Meeting of the American Society of Plastic Surgeons, April 2012, San Francisco, CA 10. Pyle JW, Angobaldo JO, Bryant AK, Marks MW, David LR. Outcomes analysis of a resident cosmetic clinic: Safety and feasibility after 7 years. Ann Plast Surg 2010;64:270-4. 11. Kreiger LM, Shaw WW. Pricing strategy for aesthetic surgery: Economic analysis of a resident clinic’s change in fees. Plast Reconstr Surg 1999;103:695-700. 12. Freiberg A. Challenges in developing resident training in aesthetic surgery. Ann Plast Surg 1989;22:184-7. 13. Bingham HG. Training in esthetic surgery: some problems encountered in a university program. Plast Reconstr Surg. 1980 Feb;65(2):227-8. 14. Schulman NH. Aesthetic surgery training: The Lenox Hill model. Ann Plast Surg 1997;38:309-14. 15 15. Linder SA, Mele JA, Capozzi A. Teaching aesthetic surgery at the resident level. Aesth Plast Surg 1996;20:351-4. 16. Zweifer M, Glasberg SB. An outcome-based study of aesthetic surgery in a clinic setting. Ann Plast Surg 2000;44:355-60. 17. Rohrich RJ. The importance of cosmetic plastic surgery education: an evolution. Plast Reconstr Surg. 2000 Feb;105(2):741-2. 18. Rao VK, Schmid DB, Hanson SE, Bentz ML. Establishing a multidisciplinary academic cosmetic center. Plast Reconstr Surg 2011;128:741e-6e. 19. Sullivan CA, Masin J, Maniglia AJ, Stepnick DW. Complications of rhytidectomy in an otolaryngology training program. Laryngoscope 1999;109:198-203. 20. Alam M. Cosmetic surgery as a revenue engine for academic dermatology. Arch Dermatol. 2000 Sep;136(9):1096-8. 21. Pusic AL, Klassen AF, Scott AM, Cano SJ. Development and Psychometric Evaluation of the FACE-Q Satisfaction with Appearance Scale: A New PatientReported Outcome Instrument for Facial Aesthetics Patients. Clin Plast Surg. 2013 Apr;40(2):249-60. 22. Pusic AL, Lemaine V, Klassen AF, Scott AM, Cano SJ. Patient-reported outcome measures in plastic surgery: use and interpretation in evidencebased medicine. Plast Reconstr Surg. 2011 Mar;127(3):1361-7. 23. Klassen AF, Cano SJ, Scott A, Snell L, Pusic AL. Measuring patient-reported outcomes in facial aesthetic patients: development of the FACE-Q. Facial Plast Surg. 2010 Aug;26(4):303-9. 24. Kosowski TR, McCarthy C, Reavey PL, Scott AM, Wilkins EG, Cano SJ, Klassen AF, Carr N, Cordeiro PG, Pusic AL. A systematic review of patient-reported outcome measures after facial cosmetic surgery and/or nonsurgical facial rejuvenation. Plast Reconstr Surg. 2009 Jun;123(6):1819-27. 25. Ching S, Rockwell G, Thoma A, Antony MM. Clinical research in aesthetic surgery. Clin Plast Surg. 2008 Apr;35(2):269-73. 26. Ching S, Thoma A, McCabe RE, Antony MM. Measuring outcomes in aesthetic surgery: a comprehensive review of the literature. Plast Reconstr Surg. 2003 Jan;111(1):469-80; discussion 481-2. 27. Miller SH. Competitive forces and academic plastic surgery. Plast Reconstr Surg 1998;101:1389-99. 28. D'Amico RA, Saltz R, Rohrich RJ, Kinney B, Haeck P, Gold AH, Singer R, Jewell ML, Eaves F 3rd. Risks and opportunities for plastic surgeons in a widening cosmetic medicine market: future demand, consumer preferences, and trends in practitioners' services. Plast Reconstr Surg. 2008 May;121(5):1787-92. 29. Pacella SJ, Comstock MC, Kuzon WM Jr. Facility cost analysis in outpatient 16 plastic surgery: implications for the academic health center. Plast Reconstr Surg. 2008 Apr;121(4):1479-88. 30. Pacella SJ. Exceptions to the Stark law: the ambulatory surgery center exemption. Plast Reconstr Surg. 2006 Sep;118(3):822-3; author reply 823. 31. Pacella SJ, Comstock M, Kuzon WM Jr. Certificate-of-Need regulation in outpatient surgery and specialty care: implications for plastic surgeons. Plast Reconstr Surg. 2005 Sep 15;116(4):1103-11; discussion 1112-3. 17 FIGURES Figure 1. Role of ACAPS member at parent institution. 35 30 25 20 15 10 5 0 program core faculty chief/chair chief/chair residency private director member and coordinator practitioner program director fellow 18 Figure 2. Distribution of years in practice for respondents. X-axis represents length of practice in years, Y-axis represents number of respondents for that time point. 7 6 5 4 3 2 1 41 38 35 31 28 26 24 22 20 18 16 14 12 10 7 5 2 0 0 19 Figure 3. Ratio of clinical practice, in terms of reconstructive vs. aesthetic. >90% reconstructive : <10% aesthetic 75% reconstructive : 25% aesthetic 50% reconstructive : 50% aesthetic 25% reconstructive : 75% aesthetic <10% reconstructive : >90% aesthetic 0 10 20 30 40 50 20 Figure 4. Length of time that RACs have been in practice at institution. X-axis represents length of practice in years, Y-axis represents number of respondents for that time point. 14 12 10 8 6 4 2 0 1 2 6 7 9 10 12 15 19 20 22 25 28 30 33 45 50 21 Figure 5. Distribution of number of patients seen in the RAC each year. X-axis represents number of patients seen per year, Y-axis represents number of respondents for that number of patients. 12 10 8 6 4 2 2,000 1,500 500 300 250 225 200 180 150 120 85 100 80 75 60 50 48 40 35 30 20 15 7 14 2 0 22 Figure 6. Distribution of number of procedures done in RAC each year. X-axis represents number of procedures, Y-axis represents number of respondents for each procedure number. 9 8 7 6 5 4 3 2 1 30 0 15 0 10 0 70 60 40 30 25 24 20 17 15 7 5 0 0 23 Figure 7. Components of RAC, in terms of locations for patient encounters. examination rooms licensed operating room minor procedure room skin care center non-licensed surgical suite 0 10 20 30 40 50 60 70 24 Figure 8. Participation of plastic surgery residents in the RAC. chief residents senior residents junior residents fellows interns 0 10 20 30 40 50 60 25 Figure 9. Responsible supervisor for trainees in RAC. full-time core faculty private practice volunteer faculty private practice paid faculty fellows 0 10 20 30 40 50 26 Figure 10. Type of resident supervision provided in RAC. 45 40 35 30 25 20 15 10 5 0 preoperative preoperative preoperative planning, planning, planning, surgical time surgical time surgical time out, all out, key out, all components, components components post-operative care none preoperative preoperative planning, planning only surgical time out 27 Figure 11. Type of Accreditation for RAC. Joint Commission none Other AAAASF 0 5 10 15 20 25 30 35 40 28 Figure 12. Malpractice Insurance Model for RACs. 50 45 40 35 30 25 20 15 10 5 0 we are self-insured we pay for standard we pay for standard and pay premiums malpractice and supplemental to a group trust insurance from a malpractice commercial carrier insurance from a commercial carrier we do not have malpractice insurance 29 Figure 13. Type of remuneration for attending surgeons who provide supervision of RACs. 35 30 25 20 15 10 5 0 nothing professional fee teaching stipend I don't know combination medical of stipend, directorship professional fee, directorship 30 Figure 14. Resources provided by practice to RAC. 60 50 40 30 20 10 0 clinic space scheduling nursing support disposable supplies capital equipment 31 operating reserve for the clinic back to the Dean of the Medical School back to the Hospital back to the Department of Surgery incentive plan for faculty to participate in the Clinic we are not profitable back to the Division/Department of Plastic Surgery residents' educational fund Figure 15. Transfer location of net income, if profit/loss statement positive 30 25 20 15 10 5 0 32 0 employee satisfaction surveys we do not assess the effectiveness of the clinic in-service exmination scores patient satisfaction surveys resident satisfaction surveys mortality and morbidity conference resident case logs Figure 16. Mechanisms to assess effectiveness of RAC. 60 50 40 30 20 10 33 Figure 17. Effect of the RAC on plastic surgery training. 90 80 70 60 50 40 30 20 10 0 enhances resident education no effect on resident education detracts from resident education 34 Figure 18. Impact of the RAC on the faculty practice. 40 35 30 25 20 15 10 5 0 neutral enhances the stature we do not have such of our practice a clinic serves as a liability for our practice 35 APPENDIX Resident Aesthetic Clinic: Best Practices Project ACAPS National Survey Distributed October, November, December 2012 The American Council of Academic Plastic Surgeons (ACAPS) would like to develop a set of guidelines that 1) define best practices of Resident Aesthetic Clinics and 2) provide recommendations on how to start and maintain such clinic, for residency programs that are interested in pursuing such an endeavor. The goal of this project is to outline the principles and practices of a successful venture, focusing on the pillars of patient safety, clinical outcomes, financial viability, research opportunities, and resident education. To help us with this important project, would you please answer the following questions? This survey should take you no longer than 10 minutes to complete. We will share the results of this project at the 2013 Spring Meeting of ACAPS. Thank you. GENERAL INFORMATION 1. What is your role as an ACAPS member (please pick the single best answer)? a. residency coordinator b. fellow c. private practitioner d. core faculty member e. program director f. chief/chair g. chief/chair and program director 2. How many years have you been in practice? _________________ 3. What ratio best describes the mix of your personal clinical practice? a. >90% reconstructive : <10% aesthetic b. 75% reconstructive : 25% aesthetic c. 50% reconstructive : 50% aesthetic d. 25% reconstructive : 75% aesthetic e. <10% reconstructive : >90% aesthetic 4. What type of residency program do you have? a. independent b. integrated c. independent and integrated 5. What type of organizational structure does your practice have? a. Division of Surgery at a Medical School b. Department of a Medical School c. Private Practice 6. Do you have a Resident Aesthetic Clinic, in which plastic surgery residents have a focused cosmetic experience with some degree of autonomy? Yes No (NOTE: if respondent answers “No” then go to survey end) OPERATIONAL DETAILS 36 7. How many years has the clinic been in practice? _____________________ 8. How many patients are seen in the Resident Aesthetic Clinic each year? _________________ 9. How many procedures are done in the Resident Aesthetic Clinic each year? _________________ 10. What are the components of your Resident Aesthetic Clinic? Please check all that apply. a. examination rooms b. skin care center c. minor procedure room d. non-licensed surgical suite e. licensed operating room EDUCATION 11. Is the Resident Aesthetic Clinic a formal rotation for your residency program? a. yes b. no 12. Which residents participate in the clinic? Please check all that apply. a. interns b. junior residents c. senior residents d. chief residents e. fellows 13. Do residents provide continuity of care for their patients? a. yes b. no 14. Who supervises your Resident Aesthetic Clinic? a. no one b. fellows c. private practice volunteer faculty d. private practice paid faculty e. full-time core faculty 15. What type of resident supervision do you provide? a. none b. preoperative planning only c. preoperative planning, surgical time out d. preoperative planning, surgical time out, key components e. preoperative planning, surgical time out, all components f. preoperative planning, surgical time out, all components, post-operative care PATIENT SAFETY 16. What type of accreditation does your Resident Aesthetic Clinic have? a. none b. Joint Commission c. AAASF d. AAAHC e. Other 17. Does the Resident Aesthetic Clinic have a list of inclusion/exclusion criteria for procedures done there? a. not applicable, because we do not do procedures at our center 37 b. c. yes no 18. Who primarily provides anesthesia for the procedures done at the Resident Aesthetic Clinic? a. not applicable, because we do not do procedures at our center b. the surgeon c. the nursing staff d. CRNA e. Anesthesiologist 19. For procedures done at the Resident Aesthetic Clinic, do patients ever stay overnight? a. not applicable, because we do not do procedures at our center b. yes c. no 20. Does the Resident Aesthetic Clinic have a Life Safety Plan? a. yes b. no c. I am not sure what that is 21. Has the Resident Aesthetic Clinic ever had a patient death in the facility? a. yes b. no 22. Has the Resident Aesthetic Clinic ever had a patient death within 30 days of the procedure? a. yes b. no 23. Has the Resident Aesthetic Clinic ever had a case of malignant hyperthermia? a. yes b. no 24. Has the Resident Aesthetic Clinic or one of its surgeons ever been involved in a lawsuit, regarding a patient treated at the clinic? a. yes b. no 25. Please describe your malpractice insurance model a. we do not have malpractice insurance b. we are self-insured and pay premiums to a group trust c. we pay for standard malpractice insurance from a commercial carrier d. we pay for standard and supplemental malpractice insurance from a commercial carrier 26. Do patients sign a waiver releasing the residents from malpractice liability or limiting damages that can be obtained? a. yes b. no FINANCIAL CONSIDERATIONS 27. Is your Resident Aesthetic Clinic financially viable? a. yes b. no c. I don’t know 38 28. What type of remuneration do the attending surgeons receive for providing oversight and supervision of the Resident Aesthetic Clinic? a. nothing b. teaching stipend c. professional fee d. medical directorship e. combination of stipend, professional fee, directorship f. I don’t know 29. Which type of patients can receive discounted fees for services provided? a. none b. employees only c. patients who respond to an advertisement or special promotional deal d. all 30. Do you charge for the initial patient consultation? a. yes b. no c. I don’t know 31. The best method for patient recruitment at our Resident Aesthetic Clinic is: a. word of mouth b. advertising c. employee discounts d. search–engine optimization e. hospital marketing f. other 32. What resources does your practice commit to the Resident Aesthetic Clinic? Please check all that apply. a. nursing support b. clinic space c. scheduling d. disposable supplies e. capital equipment 33. If profitable, where do you transfer the net income? Please check all that apply. a. we are not profitable b. operating reserve for the clinic c. back to the Division/Department of Plastic Surgery d. back to the Department of Surgery e. back to the Hospital f. back to the Dean of the Medical School g. residents’ educational fund h. incentive plan for faculty to participate in the Clinic RESEARCH AND OUTCOMES 34. How do you assess the effectiveness of the Resident Aesthetic Clinic? Please check all that apply. a. we do not assess the effectiveness of the clinic b. patient satisfaction surveys c. employee satisfaction surveys d. resident case logs e. in-service exmination scores f. resident satisfaction surveys 39 g. mortality and morbidity conference 35. Have you ever presented research, derived from the Resident Aesthetic Clinic, at a national scientific meeting? a. yes b. no 36. Have you ever published research, derived from the Resident Aesthetic Clinic, in a peerreviewed, scientific journal? a. yes b. no OVERALL SUMMARY 37. What is impact of a Resident Aesthetic Clinic on your practice? a. enhances the stature of our practice b. neutral c. serves as a liability for our practice 38. What is the effect of a Resident Aesthetic Clinic on surgical training? a. enhances resident education b. no effect on resident education c. detracts from resident education 39. If you do not have a Resident Aesthetic Clinic, are you interested in starting one? a. we already have a clinic b. yes c. no d. not sure 40. Please provide any additional comments regarding this project. _____________________________________________ 41. If you would like to be contacted, to be interviewed as part of a focus group, please leave your email address. _____________________________________________ 40