MRI Screening Questionaire
advertisement

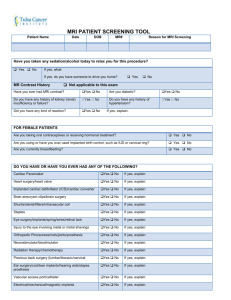
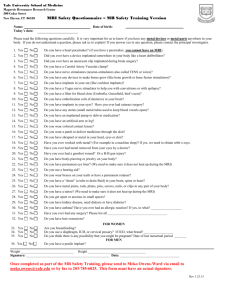
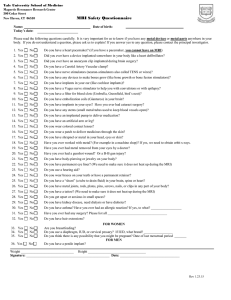
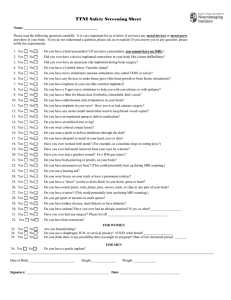
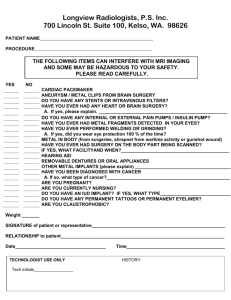
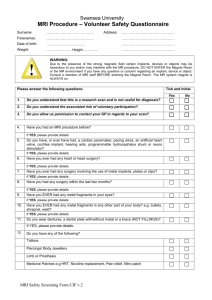
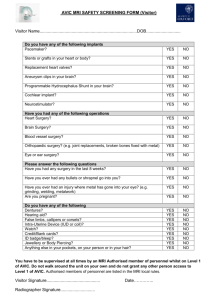
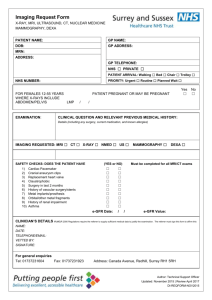
PATIENT NAME: _______________________________ Weight: ____________ DATE: ___________ MRI Screening Questionaire The following items can interfere with our MRI imaging machine and/or it can also be hazardous to your safety. Please read each question carefully and mark yes or no next to the question. You may provide comments or brief explanations on the line next to your answer. 1. Are you pregnant? Y N 3. 2. Do you have Brain Aneurysm clips? Y N Do you have a Cardiac Pacemaker or lead wires implanted? Y N 4. Do you have a Pain or Insulin pump implanted? Y N 5. Do you have a Cardiac Defibrillator or lead wires implanted? Y N 6. Do you have a Neurostimulator or lead wires implanted? Y N 7. Have you ever had metal in your eyes, or have you worked in a metal shop before? Y N 8. Have you ever had any SHRAPNEL/METAL FRAGMENTS/BULLETS in your body? Y N 9. Do you have any mechanical devices internal or external? Y N 10. Do you have any vascular clips or clamps? Y N 11. Do you have any shunts or stents? Y N 12. Do you have dentures, dental implants, braces, partial plates or bridges? Y N 13. FEMALES: Do you have an IUD or Diaphragm? Y N 14.Do you have any body piercing? Y N 15. Do you have any tattooed eyeliner, make-up or recent body tattoos? Y N 16. Do you have any metallic implants of any kind? Y N 17. Have you ever had Heart or Brain surgery before? Y N If so, what type of surgery? ______________________________________________________________________________ 18. Have you ever had ear or eye surgery before? Y N If so, what type of surgery? ______________________________________________________________________________ 19. Have you had any other types of surgery? Y N If so, what type of surgery? ______________________________________________________________________________ 20. Are you allergic to any type of medication? Y N ___________________________________ If you answered YES to any of these questions, please advice the Tech’s as soon as possible. If you have any questions, please feel free to ask the Tech’s at the time of your scan. SIGNATURE: __________________________________________ DATE:_____________________ Tel: 559.226.2888 · Fax: 559.226.2887 · 108 W. Shaw Ave · Fresno, CA 93704 · mri@mrifresno.com · www.mrifresno.com