- Molecular Testing Labs
advertisement

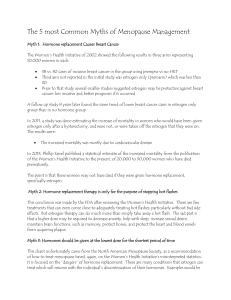
METABOLISM CLINICAL AND EXPERIMENTAL 62 (2013) S15 -S19 Available online at www.sciencedirect.com Metabolism www.metabolismjournal.com The role of personalized medicine in identifying appropriate candidates for menopausal estrogen therapy JoAnn E. Manson⁎ Brigham and Women's Hospital, Harvard Medical School ARTICLE INFO ABSTRACT Keywords: Menopausal estrogen therapy has a complex balance of benefits and risks and is no longer Personalized medicine routinely recommended for the majority of women during or after the transition to menopause. Recent findings Menopausal hormone therapy from the Women's Health Initiative (WHI) and other studies suggest that a woman's clinical and biological Estrogen characteristics may modify her health outcomes on hormone therapy (HT) and that some women may be more Progestogen appropriate candidates for therapy than others. An emerging body of evidence suggests that it may be possible to Genomics identify women who are more likely to have favorable outcomes and less likely to have adverse events on HT, as Risk stratification well as to tailor the optimal dose, formulation, and route of delivery of treatment, by the use of individual risk Clinical decision making stratification and a personalized approach. Several clinical characteristics that have been proposed for this purpose include a woman's age, time since menopause, symptom severity, baseline vascular health, risk for breast cancer, biomarker levels, and genetic predisposition. The underlying rationale for personalized medicine, that each person has a unique biologic profile that can help to guide the choice of therapy, applies well to HT decision making and holds promise for improved treatment efficacy and safety. This report, which focuses on vascular health, reviews the evidence on the role of such markers in tailoring the use of hormone therapy to appropriate candidates, with the ultimate goal of developing a personalized risk:benefit prediction model that takes into account clinical and genetic factors, "patient-centered" outcomes including sense of well being and quality of life, and other variables. The proposed personalized approach to HT decision making has the potential to improve the quality of health care. © 2013 Published by Elsevier Inc. 1. Background fits for many women [2,3]. Estrogen therapy (ET), as well as combination estrogen and progestin therapy (EPT), has complex biological effects that vary according to the clinical More than 70% of women have vasomotor symptoms during characteristics of the woman [1,4]. Thus, several clinical factors, the menopause transition and 15%-20% have moderate-tosevere symptoms that interfere with sleep and impair quality including a women's age, time since menopause, baseline vascular health, of life [1-3]. Estrogen therapy was once the mainstay of treatment for women with menopausal symptoms but recent randomized clinical trials have demonstrated that risks of menopausal to modulate her hormone therapy (HT) may outweigh the bene- several other studies provide strong support for this concept. risk for breast cancer, biomarker levels, and genetic predisposition appear health outcomes on hormone therapy [1,3,5-9]. Recent findings from the Women's Health Initiative (WHI) and Publication of this article was supported by the Collège International de Recherche Servier (CIRS). ⁎ Corresponding author. Division of Preventive Medicine, Brigham and Women's Hospital, Harvard Medical School, 900 Commonwealth Avenue East, Boston, Massachusetts 02215. Tel.: +1 617 278 0871; fax: +1 617 731 3843. E-mail address: jmanson@rics.bwh.harvard.edu. 0026-0495/$ - see front matter © 2013 Published by Elsevier Inc. http://dx.doi.org/10.1016/j.metabol.2012.08.015 S16 METABOLISM CLINICAL AND EXPERIMENTAL 62 (2013) S15 -S19 Thus, an emerging body of evidence suggests that it may be possible to identify women who are better candidates for HT, i.e., those more likely to have favorable outcomes and less likely to have 2. Cardiovascular outcomes related to menopausal hormone therapy adverse events, by the use of individual risk stratification and a personalized approach. Moreover, it may be possible to use this In the overall WHI study population, women randomized to estrogen- information to tailor decision making about the type of HT, including the progestin were 24% more likely to develop CHD optimal dose, formulation, and route of delivery, to the individual patient. unique biologic profile that can help to guide the choice of therapy, applies (defined as myocardial infarction or coronary death), 30%40% more likely to develop stroke, and at least twice as likely to develop pulmonary embolism as women assigned to placebo [11,13]. well to clinical decision making regarding HT and holds promise for Women assigned to 6.8 years of estrogen alone had a neutral risk for CHD, improved treatment efficacy and safety. a nearly 40% increase in stroke, and a nonsignificant increase in The underlying rationale for personalized medicine, that each person has a This report reviews the evidence from the WHI and other studies, pulmonary embo- lism, as compared with women assigned to placebo including work in progress, on the role of clinical characteristics, [12,14]. Recent research has elucidated several clinical characteris- tics, serum/plasma biomarkers, genomic markers, personal risk factors, and biochemical and genetic biomarkers that and gene-environment interactions, in helping to identify good versus poor candidates for HT use, with a focus on cardiovascular outcomes. This article addresses personalized care and risk indicate higher vs lower risk of adverse cardiovascular disease (CVD) stratification for hormonal interventions only among women with a clinical CVD risk while taking HT and that appear to help identify better vs worse indication for systemic HT, including vasomotor symptoms severe enough candidates for HT use are: age, time since menopause onset, LDL to interfere with sleep or impair quality of life, in conjunction with her cholesterol and other lipid levels, metabolic syndrome, and Factor V personal interest in receiving this treatment. The ultimate goal is the Leiden genotype [3,7,15]. Moreover, emerging evidence suggests that development and validation of a personalized risk: benefit prediction model women at elevat- ed thrombotic risk should either avoid systemic HT or for HT use that takes into account choose clinical and genetic factors, "patient-centered" outcomes such as subjective sense of well being and quality of life, personal preference for behavioral vs pharmacologic therapy, and other a transdermal, rather than oral, route of delivery [1-3,16]. outcomes, including CHD, stroke and venous thromboembolism (VTE), while taking HT. The strongest factors that have been found to modify 2.1. Influence of age and time since menopause variables to determine appropriateness of treatment, as well as guiding the selection of dose, formulation, and route of hormone delivery. As most of the research relevant to this report derives from the WHI, a WHI analyses suggest that age or time since menopause influences the relation between HT and CHD. In analyses pooling data across both trials, HT-associated RRs for CHD brief summary of the study design follows. The WHI HT trials included were 0.76 (95% CI 0.50-1.16), 1.10 (95% CI 0.84-1.45), and 1.28 more than 27,000 healthy postmeno- pausal women aged 50 to 79 (mean (95% CI 1.03-1.58) among women who were <10, 10-19, and 20 years past the age, 63) [10]. In the menopausal transition at study enrollment, respectively (p, trend=0.02) [5] Among estrogen-progestin trial, 16,608 women with a uterus were randomized to daily oral estrogen plus progestin (0.625 mg of women aged 50-59, estrogen alone was associated with significant reductions in conjugated equine estrogens [CEE] plus 2.5 mg of medroxy- progesterone the secondary endpoint of coronary revascularization (RR= acetate [MPA]) or a placebo [11]. In the estrogen- alone trial, 10,739 women with hysterectomy (41% also had oophorectomy) were randomized 0.55; 95% CI 0.35-0.86) and a composite endpoint of MI, coronary death, or coronary revascularization (RR=0.66; 95% to daily oral estrogen alone (0.625 mg of CEE) or a placebo [12]. The main CI 0.44-0.97), but CHD risk reductions were not seen for ages outcome of interest was coronary heart disease (CHD), so older women 60-69 or 70-79 [14]. Overall, HT appeared to have a beneficial or neutral effect on CHD in women closer to menopause (who are likely to have healthier arteries) but a harmful effect in later years were targeted for enrollment because their higher baseline coronary risk led to improved study power. The estrogenprogestin trial was terminated 3 years early (after an average of 5.6 years of treatment) because of an unfavorable risk- [6,8,9]. Analysis of the entire follow-up period (i.e., intervention plus post- benefit ratio associated with estrogen-progestin in the overall study population (increased risk of CHD, stroke, and venous thromboembolism [VTE]) and a significant increase in breast cancer risk) intervention phases) of the estrogen-alone trial also found more favorable [11]. The estrogen-alone trial was terminated ~1 year early (after 6.8 years) alone were because of an elevated risk for stroke that was not offset by a reduced risk 0.54 (0.34-0.86), 1.05 (0.82-1.35) and 1.23 (0.92-1.65) for ages 50- for CHD in the hormone group [12]. Although both regimens lowered the 59, 60-69, and 70-79, respectively (p, interaction=0.007) [17]. Results were similar for CHD [17]. risk for osteoporotic fracture and estrogen-alone was also associ- ated with an unexpected borderline significant reduction in breast cancer risk, the effects for myocardial infarction (MI) and CHD in younger, compared with older, women. For MI, the RRs associated with randomization to estrogen For stroke, no effect modification was apparent by age. risks appeared to outweigh the benefits for a large segment of the WHI Women assigned to either estrogen-progestin or estrogen study population. Cardiovas- cular health outcomes in the trials and alone were 30%-40% more likely to experience stroke than those assigned to placebo, irrespective of age [5,11,12,18]. quality of life parameters are the focus of the discussion below. Baseline age, time since menopause, and other clinical characteristics did not clearly identify women at higher vs lower risk of stroke on HT. S17 METABOLISM CLINICAL AND EXPERIMENTAL 62 (2013) S15 -S19 Table 1 - CHD Risk in the WHI HT Trials (E+P and E-Alone) According to Baseline Levels of Biomarkers. assignment to HT was associated with a 40% lower risk for CHD, while Biomarker OR (95% CI) for HT Treatment Effect P-Value ratio >2.5), assignment to HT resulted in a 73% higher risk (p-value for among women with an adverse cholesterol profile at baseline (LDL/HDL interaction =0.002) [7]. Baseline hsCRP levels were marginally predictive of LDL-Cholesterol (mg/dl) <130 0.66 (0.34-1.27) CHD risk on HT [7]. 0.03 130 1.46 (1.02-2.10) LDL/HDL Cholesterol Ratio <2.5 0.60 (0.34-1.06) 2.5 1.73 (1.18-2.53) hs-CRP (mg/dl) <2.0 1.01 (0.63-1.62) 2.0 1.58 (1.05-2.39) 0.002 0.16 Source: Bray PF, et al. Am J Cardiol 2008; 101:1599. Although several other biomarkers were predictive of CHD risk in the WHI, including lipids (high LDL cholesterol, low HDL cholesterol, high triglycerides) and higher levels of interleukin6, matrix metalloproteinase 9, D-dimer, factor VIII, von Willebrand factor, leukocyte count, homocysteine, and fasting insulin [20], only the lipid abnormalities described above significantly modified the effect of HT on CHD and helped to identify women more or less likely to have CHD events on HT. Other biomarkers are currently being studied (see Table 2 for listing of selected biomarkers under study in the WHI and other randomized trials and/or Regarding pulmonary embolism, compared with those in the placebo group, women in the estrogen-progestin group experienced a statistically significant doubling of risk [15]. Assignment to estrogen alone appeared to raise the risk by 37%; this increase was not statistically significant [19]. No clear effect modification by age or time since menopause was apparent. Lower absolute baseline risks observational studies). Extensive arrays of biomarkers are also under study for identification of women at high versus low risk of other outcomes on hormone therapy, including cancer, diabetes, cognitive decline, and autoimmune disorders, among others. Whether or not these biomarkers enhance risk stratification will be known soon. of CHD, stroke, VTE, and other adverse events in younger vs older women, however, translated 2.3. Genetic markers into much lower absolute excess risks associated with HT use in the former group. Factor V Leiden was strongly predictive of pulmonary embolism and other VTE events and the genetic polymor- 2.2. Biomarkers phism glycoprotein IIIa leu33pro predicted CHD events in WHI [15,20]. Factor V Leiden also interacted with HT to augment Lower LDL cholesterol and lower LDL/HDL ratios were strongly predictive of more favorable CHD outcomes on HT, again consistent with VTE risk [15]. However, glycoprotein IIIa leu33pro did not clearly modify better outcomes among women with lower baseline cardiovascular risk have been linked to VTE, CHD, stroke, and other cardiovascular events, [7,13] (Table 1). Among participants with a better cholesterol profile at but it remains unclear if these genetic factors interact with HT to amplify baseline (LDL/HDL ratio <2.5), risk [21]. In the WHI, estrogen receptor polymorphisms were Table 2 - Selected biomarkers under study to aid risk stratification for hormone therapy decision making. the effect of HT on vascular risk [20]. Gene variants in ABO blood group found to reduce the effect of HT on plasmin-antiplasmin, a marker of coagulation and fibrinolysis [22]. Analyses of other promising genetic markers are under study and results are expected soon (Table 2). These include gene variants related to sex hormone biosynthesis, metabolism, and signaling. Ge- nome-wide association studies (GWAS) are Biochemical Markers: • Lipids (serum LDL cholesterol, LDL/HDL ratios, triglyceride levels, Lp(a), 27-OH-Cholesterol, apolipoprotein levels) also in progress and will aid with discovery of gene variants that may modify risks of vascular events and other outcomes on HT. • Inflammatory markers (high-sensitivity C-reactive protein [hsCRP], interleukin-6, tumor necrosis factor alpha, leukocyte count) • Adipokines (adiponectin, leptin, retinol binding protein-4 [RBP4]) • Endothelial markers (E-selectin, P-selectin, ICAM, VCAM) • Glucose tolerance markers: fasting glucose, insulin, HOMA-IR, 3. Menopausal symptoms and quality of life IGF-1, and biomarkers of metabolic syndrome • Matrix metalloproteinases • Hemostatic markers (D-dimer, factor VIII, von Willebrand Women with menopausal symptoms, including hot flashes, night sweats, disrupted sleep, and vaginal or genital dryness, are more factor, homocysteine, fibrinogen, tissue factor pathway likely to derive quality-of-life benefits from HT than inhibitor or acquired activated protein C resistance) women without such symptoms. In the WHI [23-25], among • Sex steroid hormone levels, sex hormone binding globulin level Genetic Markers: • Factor V Leiden • Glycoprotein IIIa leu33pro • Gene variants in ABO blood group • Estrogen and progesterone receptor polymorphisms • Gene variants related to sex hormone biosynthesis • Gene variants related to sex hormone metabolism • Gene variants related to sex hormone signaling • Genome-wide association studies (GWAS) and exome sequencing for gene discovery women who were symptomatic at baseline, estrogenprogestin provided significantly greater relief than placebo at 1 year for hot flashes (RR=4.40; 95% CI, 3.40-5.71), night sweats (RR=2.58; 2.04-3.26), vaginal or genital dryness (RR=2.40; 1.90- 3.02), joint pain or stiffness (RR=1.43; 1.24-1.64), and general aches or pains (RR=1.25; 1.08-1.44). However, HT also had adverse effects including an increased risk of vaginal bleeding and need for dilation and curettage procedures or hysterecto- my, headaches, breast tenderness, and urinary incontinence [23-25]. A similar pattern was seen for estrogen-alone [26,27]. S18 METABOLISM CLINICAL AND EXPERIMENTAL 62 (2013) S15-S19 Research is ongoing to identify the clinical characteristics that predict a net favorable effect of HT on quality-of-life outcomes. Conflict of interest The author has nothing to disclose. 4. Dose, formulation, and route of hormone delivery REFERENCES Using lower doses, bioidentical vs synthetic formulations, and the transdermal, rather than oral, route of administration of estrogens and progestogens may result in a lower risk of side effects and adverse events [1-4]. Differences would be expected due to avoidance of the first-pass hepatic effects of oral estrogen and differences in hormone concentrations in the blood achieved by varying doses and routes of delivery. With transdermal therapy, it may be possible to avoid the increased synthesis of clotting factors, the increase in tri- glycerides, changes in C-reactive protein levels, and increases in sex hormone-binding globulin that may lower free testosterone levels and adversely affect libido. Observational evidence, although limited, suggests that transdermal estro- gen therapy may be associated with a lower risk of venous thromboembolism and stroke than oral administration [1,2,16]. Randomized clinical trial evidence, however, is lacking. Women with an increased propensity for thrombosis and higher baseline risk of vascular disease should avoid oral estrogen. It may be possible to use risk prediction models based on clinical characteristics, baseline biomarkers, and gene variants to identify women most likely to benefit from low-dose therapy or transdermal delivery, as compared with oral HT in conventional doses, or who should be advised to avoid any form of estrogen therapy. 5. Conclusions Menopausal HT has a complex balance of benefits and risks that can vary according to the clinical and biological charac- teristics of the woman. An emerging body of evidence suggests that it may be possible to identify women who are better candidates for HT, i.e., those more likely to have favorable outcomes and less likely to have adverse events, as well as to tailor the optimal dose, formulation, and route of delivery of HT, by the use of individual risk stratification and a person- alized approach. The WHI and other studies suggest an important role of clinical characteristics, serum biomarkers, genomic markers, and gene-environment interactions to attain this goal. The development of a personalized risk: benefit prediction model for HT use that takes into account clinical and genetic factors, "patient-centered" outcomes such as subjective sense of well being and quality of life, personal preference for behavioral vs pharmacologic therapy, and other variables, hold promise for improving clinical decision making and the quality of health care. Acknowledgment The author is greatful to shari Bassuk and Philomena Quinn for expert assistance. [1] North American Menopause Society. Estrogen and progestogen use in postmenopausal women: 2010 position statement of The North American Menopause Society. Menopause 2010;17:242-55. [2] Santen RJ, Allred DC, Ardoin SP, Archer DF, Boyd N, Braunstein GD, et al. Postmenopausal hormone therapy: an Endocrine Society scientific statement. J Clin Endocrinol Metab 2010;95:S1-66. [3] Manson JE, Bassuk SS. The menopause transition and postmenopausal hormone therapy. In: Longo DL, Fauci AS, Kasper DL, Hauser SL, Jamison JL, Loscalzo J, eds. Harrison's principles of internal medicine: McGraw-Hill, 2011. [4] International Menopause Society. Aging, menopause, cardiovascular disease and HRT. International Menopause Society Consensus Statement. Climacteric 2009;12:368-77. [5] Rossouw JE, Prentice RL, Manson JE, Wu L, Barad D, Barnabei VM, Ko M, LaCroix AZ, Margolis KL, Stefanick ML. Effects of postmenopausal hormone therapy on cardiovascular disease by age and years since menopause. JAMA 2007;297: 1465-77. [6] Manson JE, Bassuk SS. Invited commentary. Hormone therapy and risk of coronary heart disease: why renew the focus on the early years of menopause? Am J Epidemiol 2007;166:511-7. [7] Bray PF, Larson JC, Lacroix AZ, Manson J, Limacher MC, Rossouw JE, Lasser NL, Lawson WE, Stefanick ML, Langer RD, Margolis KL. Usefulness of baseline lipids and C-reactive protein in women receiving menopausal hormone therapy as predictors of treatment-related coronary events. Am J Cardiol 2008;101:1599-605. [8] Mendelsohn ME, Karas RH. Molecular and cellular basis of cardiovascular gender differences. Science 2005;308: 1583-7. [9] Grodstein F, Clarkson TB, Manson JE. Understanding the divergent data on postmenopausal hormone therapy. N Engl J Med 2003;348:645-50. [10] Women's Health Initiative Study Group. Design of the Women's Health Initiative clinical trial and observational study. The Women's Health Initiative Study Group. Control Clin Trials 1998;19:61-109. [11] Writing Group for the Women's Health Initiative Investigators. Risks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results from the Women's Health Initiative randomized controlled trial. JAMA 2002;288:321-33. [12] Women's Health Initiative Steering Committee. Effects of conjugated equine estrogen in postmenopausal women with hysterectomy: the Women's Health Initiative randomized controlled trial. JAMA 2004;291:1701-12. [13] Manson JE, Hsia J, Johnson KC, Rossouw JE, Assaf AR, Lasser NL, Trevisan M, Black HR, Heckbert SR, Detrano R, Strickland OL, Wong ND, Crouse JR, Stein E, Cushman M. Estrogen plus progestin and the risk of coronary heart disease. N Engl J Med 2003;349:523-34. [14] Hsia J, Langer RD, Manson JE, Kuller L, Johnson KC, Hendrix SL, Pettinger M, Heckbert SR, Greep N, Crawford S, Eaton CB, Kostis JB, Caralis P, Prentice R. Conjugated equine estrogens and the risk of coronary heart disease: the Women's Health Initiative. Arch Intern Med 2006;166:357-65. METABOLISM CLINICAL AND EXPERIMENTAL 62 (2013) S15 -S19 [15] Cushman M, Kuller LH, Prentice R, Rodabough RJ, Psaty BM, Stafford RS, Sidney S, Rosendaal FR. Estrogen plus progestin and risk of venous thrombosis. JAMA 2004;292: 1573-80. [16] Canonico M, Oger E, Plu-Bureau G, Conard J, Meyer G, Levesque H, Trillot N, Barrellier MT, Wahl D, Emmerich J, Scarabin PY. Hormone therapy and venous thromboembolism among postmenopausal women: impact of the route of estrogen administration and progestogens: the ESTHER study. Circulation 2007;115:840-5. [17] LaCroix AZ, Chlebowski RT, Manson JE, Aragaki AK, Johnson KC, Martin L, Margolis KL, Stefanick ML, Brzyski R, Curb JD, Howard BV, Lewis CE, Wactawski-Wende J. Health outcomes after stopping conjugated equine estrogens among postmenopausal women with prior hysterectomy: a randomized controlled trial. JAMA 2011;305:1305-14. [18] Wassertheil-Smoller S, Hendrix SL, Limacher M, Heiss G, Kooperberg C, Baird A, Kotchen T, Curb JD, Black H, Rossouw JE, Aragaki A, Safford M, Stein E, Laowattana S, Mysiw WJ. Effect of estrogen plus progestin on stroke in postmenopausal women: the Women's Health Initiative: a randomized trial. JAMA 2003;289:2673-84. [19] Curb JD, Prentice RL, Bray PF, Langer RD, Van Horn L, Barnabei VM, Bloch MJ, Cyr MG, Gass M, Lepine L, Rodabough RJ, Sidney S, Uwaifo GI, Rosendaal FR. Venous thrombosis and conjugated equine estrogen in women without a uterus. Arch Intern Med 2006;166:772-80. [20] Rossouw JE, Cushman M, Greenland P, et al. Inflammatory, lipid, thrombotic, and genetic markers of coronary heart disease risk in the Women's Health Initiative trials of hormone therapy. Arch Intern Med 2008;168:2245-53. [21] Carpeggiani C, Cocean M, Landi P, et al. ABO blood group alleles: a risk factor for coronary artery S19 disease. An angiographic study Atherosclerosis 2010;211: 461-6. Rossouw JE, Bray P, Liu J, et al. Estrogen receptor [22] polymorphisms and the vascular effects of hormone therapy. Arterioscler Thromb Vasc Biol 2011;31:464-9. Barnabei VM, Cochrane BB, Aragaki AK, Nygaard I, Williams [23] RS, McGovern PG, Young RL, Wells EC, O'Sullivan MJ, Chen B, Schenken R, Johnson SR. Menopausal symptoms and treatmentrelated effects of estrogen and progestin in the Women's Health Initiative. Obstet Gynecol 2005;105: 1063-73. Ockene JK, Barad DH, Cochrane BB, Larson JC, Gass M, [24] Wassertheil-Smoller S, Manson JE, Barnabei VM, Lane DS, Brzyski RG, Rosal MC, Wylie-Rosett J, Hays J. Symptom experience after discontinuing use of estrogen plus progestin. JAMA 2005;294:183-93. Hays J, Ockene JK, Brunner RL, Kotchen JM, Manson JE, [25] Patterson RE, Aragaki AK, Shumaker SA, Brzyski RG, LaCroix AZ, Granek IA, Valanis BG. Effects of estrogen plus progestin on health-related quality of life. N Engl J Med 2003;348: 1839-54. Brunner RL, Gass M, Aragaki A, Hays J, Granek I, Woods N, [26] Mason E, Brzyski R, Ockene J, Assaf A, LaCroix A, Matthews K, Wallace R. Effects of conjugated equine estrogen on healthrelated quality of life in postmenopausal women with hysterectomy: results from the Women's Health Initiative Randomized Clinical Trial. Arch Intern Med 2005;165:1976-86. Brunner RL, Aragaki A, Barnabei V, Cochrane BB, Gass M, [27] Hendrix S, Lane D, Ockene J, Woods NF, Yasmeen S, Stefanick M. Menopausal symptom experience before and after stopping estrogen therapy in the Women's Health Initiative randomized, placebo-controlled trial. Menopause 2010;17: 946-54.