1|Laser Consultation Form
ID:
#F 1 2 3 4 5 6
Office Use
Infusionsoft
Patch Test
First Appointment
Plan Type
Laser Treatments
For most people laser hair removal treatment is generally safe and effective but contraindications also need to be considered when
deciding upon laser hair removal treatment; some conditions may be made significantly worse and action may need to be taken
prior to the start of treatment course. Your treatment practitioner should be made aware of your medical history and any
medications you are currently taking before any treatment takes place. They should take this into account and use their own
experience and judgment to make the process as safe as possible for you. Also to be on the safe side you should contact your GP to
discuss if any of your medications or medical conditions will be worsened by or complicate laser hair removal treatment.
You must tell your practitioner of any recent hair removal such as waxing. This is important because in order to achieve good hair
removal results it is essential to have hair follicles. Any recent waxing and plucking of hair can remove the hair follicles and this
will prevent you from getting good results from any laser hair removal treatments.
Hirsutism
Hirsutism (the medical term for excessive body hair) can be a symptom of an underlying medical condition. Such conditions are
generally hormone related, e.g. polycystic ovarian syndrome. The first port of call if you have excessive body hair should be to your
GP, to discuss the problem and rule out any underlying health problems, which could be causing the problem.
Medical Conditions which are Contraindicative
Some medical conditions must be considered with caution.
Laser hair removal treatment can cause problems for those with active or chronic herpes simplex viral infections. Your
practitioner must know before treatment if you suffer from such an infection. You can be given antiviral medication
several days before starting treatment and this will normally continue for up to 1 week. Antiviral medication is particularly
important if you suffer from viral lesions on the area you want to have treated.
Care should also be taken if you suffer from hypertrophic scarring or keloid formation. You practitioner should use their
own judgment and advise you as you may have problems with skin healing if the skin is damaged during laser treatment.
Other conditions which should be approached with caution include psoriasis, bleeding disorders, vitiligo and severe
histamine reactions.
Laser hair removal treatment should not be carried out on skin which is sunburnt, or had surgeries such as laser
resurfacing and chemical peels. Laser hair removal will not be conducted over tattoo’s.
You cannot be treated if you are pregnant.
You cannot be treated if you are undergoing chemotherapy or have a history of skin cancer.
You cannot be treated if you have auto immune conditions - Lupus etc
Medication which is Contraindicative
Certain types of medication can affect laser hair removal treatment and any healing periods afterwards.
If you are currently taking isotretinoin (or Accutane as it is commercially known), you should stop taking this 6 months
before undergoing laser hair removal treatment. This drug can cause skin sensitivity and this is not beneficial in laser hair
removal treatment.
Photosensitising drugs that are activated by ultraviolet A light wavelengths may also contraindicate some laser hair
removal treatments. If you are taking such medication it is safer to use laser treatments, which work within the visible and
infrared parts of the light spectrum.
There are a multitude of common drugs, which can also interfere with treatment. Steroids, antibiotics such as
tetracyclines and analgesics like ibuprofen are just some such drugs. Y mustn't take Ibuprofen (ie Nurofen as an example
brand) for 7 days prior to your appointments.
St Johns Wort
2|Laser Consultation Form
ID:
Surname
First Name
Mr/Mrs/Miss/Other
DOB
/
/
Home Address
Postcode
Work Tel No
Home Tel No
Mobile Tel No
Email
Doctor’s Name & Address
Emergency Contact Name & Phone Number
Ethnic origin
Treatment Requested (please circle)
Occupation
Hair Removal / Vascular / Fungal Nail
Other
Area(s)
Lifestyle & medical History – please tick for yes or cross for no in every circle as appropriate.
If you do not understand or recognise the condition then please discuss with your Laser operator.
Pregnant (or planning pregnancy)
PCOS/Hormonal Imbalance
Sun tanned/Using sun beds or fake tan
Thyroid Condition
Skin Pigmentation Disorders (e.g. melasma, vitiligo)
Regular Smoker
History of cancer (or chemo/radio therapy)
Psoriasis/Eczema
Diabetes
Depression/Anxiety
Epilepsy
Herpes (Shingles/Cold sores)
Lymphatic/Immune System Disorders
High Blood Pressure
History of Keloid formation/scarring
Photosensitive conditions
Lupus
Allergies
Communicable Conditions (Hepatitis/HIV)
Units alcohol/week
3|Laser Consultation Form
ID:
Are you:
Currently taking any medication or any supplements?
No/Yes (please specify the condition & medications)
Currently using/used in the last 3 months, any of the following? I n n o n e c i r c l e N O h e r e (please circle)
St John’s Wort / Amiodarone / Tetracycline Antibiotics / Anticoagulants / Oral or Topical
Retinoids (e.g. Roaccutane or Retin A) / Oral or Topical Steroids
Comments:
Recovering from any major medical treatment or photodynamic therapy (PDT) within the last 6 months?
No/Yes (please specify)
Has the area for treatment:
Ever had any of the following? (please circle) If none circle NO here
Moles / Birthmarks / Tattoos / Permanent makeup / Chemical peel / Botox / Inject able fillers /
Suffered from any skin disorder/disease?
Had previous Laser or IPL treatment?
No / Yes
No
/ Yes
Your skin:
What products do you use on your skin?
Please indicate how your skin responds to midday summer sun exposure with no sunscreen:
Skin Type 1 Always burns, never tans
Skin Type 2 Easily burnt, eventually gets a moderate tan
Skin Type 3 Sometimes burns, quickly gets an average tan
Skin Type 4 Rarely burns, quickly gets a deep tan
Skin Type 5 Very rarely burns, consistent tan
Skin Type 6 Never burns, consistent tan
Do you currently have a real or fake tan?
No / Yes
Have you had any sun exposure or sun beds in the last 4 weeks?
What are your goals/expectations for the treatment?
No / Yes
None
4|Laser Consultation Form
ID:
Pre Treatment Check List To be completed by the therapist
(Tick to confirm points have been discussed)
How treatment works
Likely clinical outcome
Pre/Post treatment care
SPF Advice
Sensation during treatment
Typical no. of treatments/interval
Possible side effects
Cost after sessions are finished
Any further questions/Comments
Informed Consent for LASER Treatment
Please read this consent form and tick each box to indicate you understand and accept the information contained herein.
The information I have given is correct to the best of my knowledge, and I have not withheld any known medical state or
condition. I will inform the Laser operator before treatment if there has been any change (for example in medications taken).
I understand that the results from this treatment vary considerably and a small percentage of people will not respond
satisfactorily to treatment.
I understand multiple treatments are necessary to achieve satisfactory results.
I understand there is no guarantee of permanent results and maintenance treatments may be necessary.
I understand that I must avoid sun exposure on the treated area for the duration of the treatment (and for up to 1 month
afterwards) or use a high sun protection factor to avoid sun damage.
I understand that there may be short-term side effects such as reddening, bruising, swelling, mild burning or blistering,
Hypo-pigmentation, (lightening of the skin) or hyper-pigmentation, (darkening of the skin), as well as rare side effects such as
scarring and permanent discolouration.
I understand that there are certain risks associated with LASER and they include but are not limited to: redness, localised
swelling and mild tenderness. Although rare, adverse effects such as light burns, blister and bruises may occur. On occasion
Laser treatment may cause pigmentation changes to the skin.
I understand that I must wear protective eye goggles to prevent damage from the laser.
I understand I must shave body parts for treatment 1 or 2 days before each session. I also understand that if areas are not
shaved, the clinic is unable to continue with session and this will count as 1 session.
I understand no waxing, plucking in certain cases hair removal cream between treatments.
I understand I have been quoted the following:
Area
Per session
Area
Per session
Area
Per session
I certify that I have read and understood all the information and my questions have been answered
before signing this consent form. I consent to the terms of this agreement.
Client Name
Client Signature
Operator Signature
Date
5|Laser Consultation Form
ID:
Laser Consultation Form
ID:
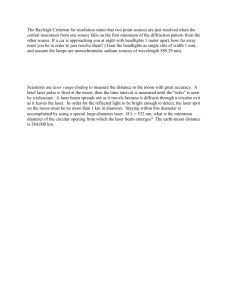
Treatment Assessment (to be completed by the operator)
Laser Consultation Form
I certify that the area highlighted above is where I have opted for treatment.
Client Name
Client Signature
6|Laser Consultation Form
ID:
Clinic Use Only ID:
1
2
3
4
5
6
7
8
9
10 11 12 13
Date
HR/Vascular
Treatment Energy
Counter before/after
Shots
Redness: 0 - 4
Swelling: 0 - 4
Sensitivity: 0 - 4
Client Initial
Therapist Initial
Additional Information
There have been no changes to my health history since my last treatment and I am not taking any new medication.
Date
Signature
Print name
Date
Signature
Print name
Date
Signature
Print name
Date
Signature
Print name
Date
Signature
Print name
Date
Signature
Print name
Date
Signature
Print name
Date
Signature
Print name
Date
Signature
Print name
Date
Signature
Print name
Date
Signature
Print name
Date
Signature
Print name
 0
0