Original paper A comparative study on the concomitant
advertisement

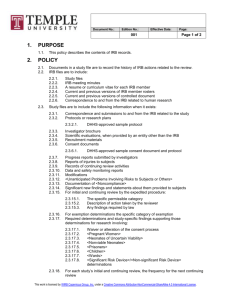
Original paper A comparative study on the concomitant administration of 5 mg amlodipine and 100 mg irbesartan and concomitant administration of 1 mg of trichormethiazide and 100 mg irbesartan Yoshio Iwashima 1), Yuko Oota 1), Shinichiro Hayashi 1), Takeshi Horio 2), and Yuhei Kawano 1) Introduction It has been found that proactive blood pressure reduction is efficacious in prevention of cardiovascular disease (CVD) due to hypertension, and the Hypertension Treatment Guidelines 2009 (JSH2009) 1) state that it is important to evaluate home blood pressure for 24-hours in addition to consultation-room blood pressure, with the aim of achieving strict blood pressure reduction treatment over 24 hours. Blood pressure reduction targets are rarely achieved through only monotherapy with an antihypertensive agent in in everyday consultation and treatment 2). JSH2009 states that if a monotherapy does not sufficiently reduce blood pressure, it is recommended to increase the dosage of the drug or change it to another antihypertensive agent with a different mechanism of action, or change to concomitant administration with the drug and one with a different mechanism of action. From amongst antihypertensive drugs, reninangiotensin (RA) system inhibitors are positioned as first-line drugs for cases suffering from complications involving the heart, kidneys, or brain, or diabetes 1). Drugs to be added to RA system inhibitors if these are not sufficiently efficacious in to achieving blood pressure reduction targets are in most cases calcium blockers (CCBs) or diuretics. The present study compared and investigated the antihypertensive effect and changes in electrolytes, endocrine/metabolic parameters, and kidney function between the concomitant use of 5 mg of amlodipine, a CCB, with 100 mg of irbesartan, an angiotensin II receptor blocker, and the concomitant administration of 1 mg of trichormethiazide, a thiazide diuretic, with 100 mg of irbesartan in patients suffering from idiopathic hypertension with insufficient antihypertensive effect from the oral administration of RA system inhibitors. I Subjects and methods 1. Subjects Subjects were 29 patients suffering from idiopathic hypertension who were undergoing treatment at the National Cerebral and Cardiovascular Center on an outpatient basis and who had not achieved target blood pressure both/either in terms of consultation-room blood pressure and/or home blood pressure through the oral administration of RA system inhibitors, and who had not already taken any CCB or diuretic. 2. Methods The observation and investigation schedule for the present study is shown in Figure 1. The study employed a crossover method with three months in each arm. 1) National Cerebral and Cardiovascular Center 2) General Internal Medicine Department 3, Kawasaki Hospital, Kawasaki Medical School Therapeutic research vol. 34 no. 6 2013 787 Allocation Observation period 3 months Drug crossover Study period 3 months n = 14 AML 5 mg + IRB 100 mg TCZ 1 mg + IRB 100 mg RA system inhibitors n = 15 TCZ 1 mg + IRB 100 mg AML 5 mg + IRB 100 mg Antihypertensive drugs other than RA system inhibitors Blood pressure measurement Blood pressure measurement Blood pressure measurement Blood/ urine collection Blood/ urine collection Blood/ urine collection Figure 1 Research protocol RA: Renin-angiotensin AML 5 ml + IRB 100 mg: 5 mg of amlodipine and 100 mg or irbesartan TCZ 1 mg + IRB 100 mg: 1 mg of trichormethiazide and 100 mg irbesartan The RA system inhibitor was changed to the concomitant use of 5 mg of amlodipine and 100 mg of irbesartan (AML + IRB) or the concomitant use of 1 mg of trichormethiazide and 100 mg of irbesartan (TCZ + IRB). Three months later, drugs were switched in both groups, one from AML + IRB to TCZ + IRB, and the other from TCZ + IRB to AML + IRB; and after the switchover, administration was continued for three months. There was no washout period before or after the switchover. Consultation-room blood pressure was measured and blood and urine examinations were performed at the time of drug switchover, at Month 3 and at Month 6. No orally administered drugs were changed, including antihypertensive agents other than RA system inhibitors, during the study period. Consultation-room blood pressure was measured three times at intervals of 1 to 2 min in a seated position following rest for 5 min or longer, and heart rate was measured for 1 min. A device based on the brachial cuff oscillometric method was used in measuring home blood pressure, and measurement was carried out twice per day during fasting within one hour of waking in the morning and before going to bed. Evaluation was performed for the average value for the 5 days prior to the hospital visit. Blood and early morning urine were sampled while subjects were in a fasting condition on each hospital visit day, and metabolic and endocrine system parameters (sodium, potassium, total cholesterol, LDL cholesterol, serum uric acid, hemoglobin A1c [HbA1c (NGSP)], fasting blood glucose, insulin, creatinine, protein urine, urinary albumin, and brain natriuretic peptide (BNP) were measured and the HOMA-index (Homoeostasis model assessmentinsulin resistance) and the CKD-EPI (chronic kidney disease epidemiology collaboration) formula 3, 4) were used to obtain the estimated glomerular filtration rate (eGFR). Patients were diagnosed with diabetes 5) or chronic kidney disease (CKD) 6) based on relevant guidelines. Antihypertensive agents were administered once a day in the morning through oral administration. The achievement of target blood pressure was evaluated using systolic blood pressure (SBP) of consultation-room blood pressure and home blood pressure based on JSH2009, and the goals in terms of consultation-room blood pressure and home blood pressure respectively were below 130 mmHg and below 125 mmHg for young/middle-aged subjects; below 140 mmHg and below 135 mmHg for elderly subjects; below 130 mmHg and 125 mmHg for patients suffering from diabetes/CKD; and below 140 mmHg and 135 mmHg for those suffering from cerebrovascular disorders 1). The present study was approved by the institutional review board of the National Cerebral and Cardiovascular Center. 3. Statistical methods Values in each measurement item were recorded using means +/- SD or actual values. In comparing changes in continuous variables from the time prior to the change, and in comparisons between continuous variables, a corresponding Student’s t-test was employed. 788 Therapeutic research vol. 34 no. 6 2013 Table 1 Subject backgrounds Age (years) Gender (m/f) (n) Hypertension history, years Smoker/ non-smoker, gave up smoking, smoker CVD history (n) Myocardial infarction Cerebral infarction Diabetes (n) CKD (n) BMI (kg/m2) Antihypertensive agents No. of administered drugs 60.8 +/- 14.1 13/16 16.7 +/- 12.7 20/8/1 Breakdown of administered drugs Renin-angiotensin system inhibitors (n) irbesartan 100 mg (n) enalapril 10 mg (n) 29 7 2 2 3 3 12 25.2 +/- 3.9 olmesartan 20 mg (n) 6 candesartan 8 mg (n) 3 temocapril 5 mg (n) 3 valsartan 80 mg (n) 7 losartan 50 mg (n) 1 Beta blockers (n) 5 1.3 +/- 0.5 Alpha blockers (n) 1 Aldosterone antagonists (n) 2 Mean values +/- SD or actual numbers, CVD: cardiovascular disease, CKD: chronic kidney disease, BMI: body mass index The blood pressure target achievement rate was calculated based on each blood pressure value, and each blood pressure target achievement rate was compared using a Chi-squared test. Levene’s test was employed in examining equal variance. Results with p < 0.05 were taken to be significant. II Results 1. Patient backgrounds Patient backgrounds are shown in Table 1. The total number of subjects was 29, with an average age of 60.8 years, and there were 13 males. Two subjects had suffered from myocardial infarction, three had a cerebral infarction, three were complicated with diabetes, and 12 with CKD. Moreover, RA system inhibitors were administered to all subjects, beta-blockers to 5 subjects, an alpha blocker to one subject, and aldosterone antagonists to 2 patients. The breakdown of RA system inhibitors prior to drug switchover was irbesartan in 7 subjects, enalapril in 2, olmesartan in 6, candesartan in 3, temocapril in 3, valsartan in 7, and losartan in 1. 2. Hypotensive efficacy Blood pressure prior to drug switchover and change in blood pressure after switchover are shown in Table 2. Six out of 29 subjects (20.7%) achieved their blood pressure reduction targets in the consultation-room blood pressure prior to switchover, there were no subjects (0%) who achieved morning home blood pressure, and there were three subjects (10.3%) who achieved bedtime home blood pressure. After drug switchover, blood pressure other than diastolic consultation-room blood pressure (p = 0.07) in subjects after administration of TCZ + IRB was significantly reduced. There was no significant change in consultation room heart rate in either treatment group between before drug switchover and after it. Moreover, there were no side effect symptoms and adverse events accompany drug switchover. 3. Change in electrolytes, endocrine/ metabolic parameters, and renal function There were no significant changes in either body weight or HbA1C after AML + IRB administration and after TCZ + IRB compared to prior to drug switchover; however, protein urine, urine albumin, and BMP were significantly reduced. After AML + IRB administration, total cholesterol, LDLcholesterol, and uric acid were significantly reduced, and eGFR was significantly elevated. Meanwhile, after TCZ + IRB administration, sodium, potassium, and eGFR were significantly reduced, and the HOMA index significantly increased (Table 2). 4. Comparison between AML + IRB and TCZ + IRB A comparison in the hypotensive efficacy between the two administration groups found no significant difference in any of the consultation-room blood pressure, early morning home blood pressure, or bedtime home blood pressure (Table 3). The blood pressure reduction target achievement rate after drug switchover significantly increased both after AML + IRB administration and after TCZ + IRB administration (Figure 2). There was no significant difference in the achievement rate between the two administration groups in any of consultation-room blood pressure (p = 0.28), early morning home blood pressure (p = 1.00) and bedtime home blood pressure (p = 0.06). Testing of the equal variance of SBP after drug switchover found no significant difference between the two treatment groups in consultation room SBP and in early morning home SBP; however, there was a significant difference in bedtime home SBP (Figure 3A –C). Table 2 Bodyweight, endocrine/ metabolic parameters and renal function prior to change; and change after switchover to AML 5 mg + IRB 100 mg or to TCZ 1 mg + IRB 100 mg Consultation-room blood pressure SBP (mmHg) DBP (mmHg) HR (bpm) Early morning home blood pressure SBP (mmHg) DBP (mmHg) Bedtime home blood pressure SBP (mmHg) DBP (mmHg) Body weight (kg) Serum sodium (mEq/L) Serum potassium (mEq/L) Total cholesterol (mg/dL) LDL cholesterol (mg/dL) Serum uric acid (mg/dL) HbA1c (%) HOMA Index eGFR (ml/min/1.73m2) Protein urine >= + 1 (n) Urine albumin (mg/g Cr) [SYMBOL] BNP (pg/ml) [SYMBOL] Before switchover Amount of change from before switchover AML 5 mg + IRB 100 TCZ 1 mg + IRB 100 mg mg 143 +/- 16 83 +/- 13 76 +/- 13 - 18.0 +/- 8.5 + - 8.0 +/- 7.5 + - 4.4 +/- 11.3 - 14.6 +/- 14.2 + - 3.7 +/- 10.7 - 3.0 +/- 15.0 145 +/- 10 86 +/- 11 - 18.8 +/- 10.1 + - 10.2 +/- 8.3 + - 17.8 +/- 12.0 + - 7.7 +/- 7.2 + 142 +/- 11 86 +/-12 65.5 +/- 14.2 141 +/- 2 - 18.3 +/- 12.1 + - 10.3 +/- 7.6 + 0.0 +/- 1.7 + 0.2 +/- 2.0 + - 13.1 +/- 14.8 + - 8.6 +/- 7.8 + 0.1 +/- 1.7 - 1.2 +/- 1.9 + 4.3 +/- 0.4 - 0.02 +/- 0.38 - 0.26 +/- 0.39 + 206 +/- 43 - 13.6 +/- 21.3 + 1.0 +/- 25.4 121 +/- 40 - 12.3 +/- 23.2 + 4.2 +/- 21.4 6.22 +/- 1.56 - 0.51 +/- 0.62 + 0.18 +/- 0.69 5.49 +/-0.64 4.34 +/-4.85 71.1 +/- 19.7 7 - 0.07 +/- 0.20 - 1.04 +/- 2.77 1.70 +/- 2.78 + -4+ 0.05 +/- 0.18 1.35 +/- 3.53 * - 3.12 +/- 4.72 + -3+ 95.2 +/- 145.7 - 60.5 +/- 109.7 + - 62.5 +/- 115.7 + 45.2 +/- 48.7 - 14.4 +/- 22.8 + - 18.9 +/- 26.0 + Mean values +/- SD or actual numbers. *: p< 0.05, +: p< 0.01 vs. prior to change (paired t test), [SYMBOL]: Compared after log-conversion. AML: amlodipine, IRB: irbesartan, TCZ: trichormethiazide, SBP: systolic blood pressure, DBP: diastolic blood pressure, LDL: low density lipoprotein, HOMA: Homoeostasis model assessment, eGFR: estimated glomerular filtration rate, BNP: brain natriuretic peptide A comparison of the two administration groups in terms of changes in electrolytes, and endocrine/metabolic parameters and renal function found significant differences in total cholesterol, LDL-cholesterol, serum uric acid, HbA1C, HOMA index, sodium, potassium, eGFR, urine albumin, and BMP (Table 3). III Discussion Subjects were patients suffering from idiopathic hypertension who had not achieved their target blood pressure in terms of consultation-room blood pressure and/or home blood pressure through the use of oral administration of drugs including IRB. A crossover method was employed, in which the concomitant administration of 5 mg of amlodipine and 100 mg of irbesartan was switched to that of 1 mg of trichormethiazide and 100 mg of irbesartan, and the administration was continued for three months before and after switchover. Although there were no adverse events observed accompanying the switchover, and no significant differences in hypotensive efficacy in terms of systolic and diastolic blood pressure from the time of switchover, nor in the blood pressure target achievement rate, the concomitant administration of 5 mg of amlodipine and 100 mg of irbesartan did not have an impact on electrolytes and glucose metabolism relative to the concomitant administration of 1 mg of trichormethiazide and 100 mg of irbesartan, and the former combination improved lipid metabolism, uric acid, and eGFR. Meanwhile, the concomitant administration of 1 mg of trichormethiazide and 100 mg of irbesartan, compared to that of 5 mg of amlodipine and 100 mg of irbesartan, improved urine albumin and BNP. 790 Therapeutic research vol. 34 no. 6 2013 Table 3 A comparison of the hypotensive effect and change in consultation-room heart rate, endocrine/ metabolism parameters, and renal function after administration of AML 5 mg + IRB 100 mg and TCZ 1 mg + IRB 100 mg Difference after change (AML 5 mg + IRB 100 mg - TCZ 1 mg + IRB 100 mg) p Consultation-room blood pressure SBP (mmHg) - 3.4 +/- 12.2 (-15.0, 4.0) 0.28 DBP (mmHg) - 4.2 +/- 8.9 (-10.0, 1.0) 0.09 Early morning home blood pressure SBP (mmHg) - 1.1 +/- 8.1 (-8.0, 5.3) 0.72 DBP (mmHg) - 2.5 +/- 8.0 (-8.5, 2.0) 0.22 Bedtime home blood pressure SBP (mmHg) -5.2 +/- 13.0 (-17.1, 6.0) 0.15 DBP (mmHg) - 1.6 +/- 6.9 (-6.6, 3.2) 0.42 Serum sodium (mEq/L) 1.41 +/- 1.94 (0.0, 3.0) < 0.01 Serum potassium (mEq/L) 0.23 +/- 0.33 (0.10, 0.45) < 0.05 Total cholesterol (mg/dL) - 14.6 +/- 19.0 (-25.0, -1.0) < 0.05 LDL cholesterol (mg/dL) - 16.5 +/- 24.1 (-23.0, -4.5) < 0.01 Serum uric acid (mg/dL) -0.90 +/- 0.61 (-1.3, -0.4) < 0.01 HbA1c (%) -0.18 +/- 0.19 (-0.25, -0.1) < 0.01 HOMA Index -2.39 +/- 3.27 (-2.92, -0.43) < 0.01 eGFR (ml/min/1.73m2) 4.82 +/- 5.02 (1.79, 6.69) < 0.01 Urine albumin (mg/g Cr) 2.05 +/- 27.89 (0.05, 7.00) < 0.05 [SYMBOL] BNP (pg/ml) [SYMBOL] 4.56 +/- 9.55 (0.05, 8.25) < 0.05 Mean values +/- SD or actual numbers (95% confidence interval), [SYMBOL]: Compared after logconversion. AML: amlodipine, IRB: irbesartan, TCZ: trichormethiazide, SBP: systolic blood pressure, DBP: diastolic blood pressure, LDL: low density lipoprotein, HOMA: Homoeostasis model assessment, eGFR: estimated glomerular filtration rate, BNP: brain natriuretic peptide RA system inhibitors, particularly, ARB, are often used in in antihypertensive treatment. The concomitant administration of CCP and RA system inhibitors has an additive hypotensive efficacy relative to monoadministration of each 7-9), does not deteriorate glucose/lipid metabolism related items, and has been found to have a renal protective effect 10-12). Also, the side-effects of CCB are lower limb edema due to expansion of peripheral arteries (elevation of capillary blood pressure); but RA system inhibitors reduce capillary blood pressure by expanding them, therefore, it can be expected that the concomitant use of CCB and RA system inhibitors will improve edema 13). Further, the concomitant administration of diuretics with ARBs enhances the hypotensive efficacy of both, and offsets side-effects such as progression of sodium sensitivity and hyperkalemia due to RA inhibitors. Thus, it is believed that the concomitant administration of hypotensive drugs used in the present study is a favorable combination 1). Irbesartan has stronger binding to AT1 receptors, which are angiotensin II receptors, and it is expected that it has a long-lasting hypotensive efficacy 14). Both the concomitant administration of amlodipine and irbesartan 15-17) and that of thiazide diuretics and irbesartan 18,19) have high hypotensive efficacy. While the present study did not find a significant difference in hypotensive efficacy and the rate of blood pressure reduction target achievement between AML + IRB and TCZ + IRB, relative to AML + IRB, there was a significantly greater variance in TCZ + IRB bedtime home SBP after drug switchover. Therapeutic research vol. 34 no. 6 2013 791 Consultation-room blood pressure Figure 2 + Early morning home blood pressure Bedtime home blood pressure Target blood pressure achievement rate after switchover : p < 0.01 vs. before switchover AML 5 mg + IRB 100 mg: amlodipine 5mg + irbesartan 100 mg TCZ 1 mg + IRB 100 mg: trichormethiazide 1 mg + irbesartan 100 mg Consultation-room systolic blood pressure Before switchover AML 5 mg + IRB 100 mg Figure 3A Before switchover TCZ 1 mg + IRB 100 mg Change in consultation-room systolic blood pressure Mean values +/- SD, +: p < 0.01 vs. before switchover AML 5 mg + IRB 100 mg: amlodipine 5mg + irbesartan 100 mg TCZ 1 mg + IRB 100 mg: trichormethiazide 1 mg + irbesartan 100 mg 792 Therapeutic research vol. 34 no. 6 2013 Home early morning systolic blood pressure Before switchover AML 5 mg + IRB 100 mg Figure 3B Before switchover TCZ 1 mg + IRB 100 mg Change in home early morning SBP Mean values +/- SD, +: p < 0.01 vs. before switchover AML 5 mg + IRB 100 mg: amlodipine 5mg + irbesartan 100 mg TCZ 1 mg + IRB 100 mg: trichormethiazide 1 mg + irbesartan 100 mg Home bedtime systolic blood pressure Before switchover AML 5 mg + IRB 100 mg Figure 3C Before switchover TCZ 1 mg + IRB 100 mg Change in home bedtime SBP Mean values +/- SD, +: p < 0.01 vs. before switchover AML 5 mg + IRB 100 mg: amlodipine 5mg + irbesartan 100 mg TCZ 1 mg + IRB 100 mg: trichormethiazide 1 mg + irbesartan 100 mg Therapeutic research vol. 34 no. 6 2013 793 TCZ + IRB may significantly vary in hypotensive efficacy for bedtime blood pressure amongst individuals relative to AML + IRB. While TCZ + IRB was not found to have an impact on lipid metabolism and uric acid, the combination reduced sodium and potassium, and elevated the HOMA index, an index of insulin resistance. There have been concerns over diuretics, particularly thiazide diuretics, having an impact on electrolytes, and lipid metabolism, glucose metabolism and uric acid 1). There is a report that the concomitant administration of 150 mg / day of irbesartan and a low-dose (12.5 mg/day) of hydrochlorothiazide (HTCZ), a thiazide diuretic, did not deteriorate glucose/lipid metabolism 20); however, the concomitant administration of 100 mg of irbesartan and 1 mg of trichormethiazide could not offset the impact on glucose metabolism, and may have caused progression of insulin resistance. Further, AML + IRB improved lipids and reduced uric acid. Irbesartan has a function of activating PPAR-γ, which is involved in insulin resistance and glucose metabolism 21), and there is a report on its effect of improving glucose and lipids 22) and that of reducing uric acid 23). Since CCB has little impact on glucose/ lipid / electrolyte metabolism, it is assumed that the concomitant administration of the drug with amlodipine helped irbesartan improve glucose and lipids, and to reduce uric acid. There have been reports that irbesartan has a function of improving left ventricular dilation 24) and heart hypertrophy retraction 25), reducing albumin urine 26), and has a renal protective function independent of hypotensive efficacy 27). eGFR, a renal function marker, improved with AML + IRB, but it deteriorated with TCZ + IRB; however, BMP and trace urine albumin, which are cardiac/ renal disorder markers, reduced after treatment, but the degree of reduction was greater with TCZ + IRB compared to with AML + IRB. It has been found that the concomitant administration of RA system inhibitors and thiazide diuretics has a greater albumin urine reduction effect compared to the coadministration of RA system inhibitors and CCB 28). Studies to date, including the NICE-Combi study 12), in which the concomitant administration of controlled-release nifedipine and candesartan was compared to ARB monotherapy in patients suffering from idiopathic hypertension; and the BENEDICT study 29), in which the effect of the monoadministration and concomitant administration of the angiotensin converting enzyme (ACE) inhibitors trandolapril and verapamil were compared with placebo in patients suffering from hypertension complicated with type II diabetes without renal disorder, found that the concomitant administration of CCB and RA system inhibitors has a renal protective effect. Guidelines issued in recent years by Kidney Disease: Improving Global Outcomes rate the severity of kidney disease using both eGFR and albumin urine 6) . Therefore, no conclusion has been reached on the relative advantages in terms of kidney protective effects between the concomitant administration of AML + IRB and TCZ + IRB; rather, both combinations may be effective in protecting the kidneys. Conclusion Switchover to the concomitant administration of 5 mg of amlodipine and 100 mg of irbesartan resulted in favorable hypotensive efficacy in patients suffering from idiopathic hypertension who did not achieve their target blood pressure in terms of consultation-room blood pressure and/or home blood pressure through the oral administration of ARB. Relative to the concomitant administration of 1 mg of trichormethiazide and 100 mg of irbesartan, the former combination did not have an impact on electrolytes and glucose metabolism, improved lipid metabolism and uric acid, and a possibility was suggested that this concomitant administration has cardio-protective and renal-protective effects. An adjuvant tablet of 5 mg of amlodipine and 100 mg of irbesartan (Aimix® adjuvant tablet LD) has been launched on the market, and it is believed that this product is an effective alternative for patients suffering from hypertension who did not achieve the target blood pressure through ARB monotherapy. References 794 Therapeutic research vol. 34 no. 6 2013 16) Kazuyuki Shimada, Kazunari Komuro, Hiroaki Matsubara, Yukiya Murata, Kenji Kawauchi. An investigation into the efficacy and safety of the concomitant administration of irbesartan and amlodipine: A multi-facility randomized double-blind parallel group comparative study in patients suffering from idiopathic hypertension with insufficient hypotensive effect through monotherapy. Ketsuatsu 2011; 18 (12) 1231-43. 17) Kazuyuki Shimada, Kazunari Komuro, Hiroaki Matsubara, Naoko Yamamoto, Kenji Kawauchi. An investigation into the efficacy and safety of the adjuvant of irbesartan and amlodipine (Aimix® adjuvant tablet LD, HD): a multifacility long-term administration study in patients suffering from idiopathic hypertension with insufficient hypotensive effects through monotherapy. Ketsuatsu 2012; 19 (11): 1022 - 34 Therapeutic research vol. 34 no. 6 2013 795 (Paper accepted on May 13, 2013) 796 Therapeutic research vol. 34 no. 6 2013