Jesse Tyma paper 2014 - eCommons@Cornell
advertisement

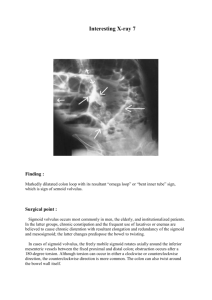
Surgical Correction of Large Colon Volvulus and Colopexy in a Postpartum Mare Jesse Tyma Clinical Advisor: Dr. Hayley Lang Pre-Clinical Advisor: Dr. Susan Fubini Senior Seminar Paper Cornell University College of Veterinary Medicine January 22, 2014 Abstract: A 17-year old Thoroughbred broodmare presented to the Cornell Large Animal Emergency Service on 6/12/13 for colic five weeks post-partum. On presentation, the mare was quiet, alert, responsive, and moderately painful. Vital signs were normal and the patient’s abdomen was distended with minimal gastrointestinal sounds auscultable. Rectal examination revealed a gas-distended viscus in the right caudal abdomen and tight bands coursing transversely. Transabdominal ultrasound showed diffusely thickened colon walls and colonic mesenteric vessels positioned against the right body wall. An exploratory celiotomy revealed a 360° large colon volvulus entrapping the cecum. The large colon was diffusely edematous but relatively non-compromised; it was decompressed and replaced in the abdomen and a colopexy was performed from the ventral band of the left ventral colon to the body wall. The patient was treated post-operatively with intravenous fluids, plasma, Lidocaine, antibiotics, antiinflammatories, anti-endotoxic agents, and precautions were taken to attempt to prevent laminitis. The patient recovered well and was discharged from the hospital six days following surgery, but later returned due to an incisional infection and substantial weight loss. These resolved with wound therapy and dietary modifications. This case report will describe the workup and treatment of this patient for a large colon volvulus that was surgically corrected and followed with a colopexy. In addition, diagnostics for colic, surgical treatment options for large colon volvulus, and postoperative concerns for the large colon volvulus patient will be described. History and Signalment: A 17-year old, five-week-postpartum Thoroughbred mare presented to the Cornell Large Animal Emergency Service on 6/12/13 for a three-hour history of colic. The mare received Page | 2 Flunixin meglumine and was sedated several times with Detomidine, but persistently brokethrough with more painful signs. At the time of workup by the referring veterinarian, the mare was tachycardic, no net reflux was obtained upon nasogastric tube placement, tight bands were palpated on rectal examination, and ultrasound of the right abdominal wall revealed enlarged colonic vessels. The foal was weaned and the mare was shipped to Cornell with a nasogastric tube in place. Seven months prior, the mare had surgical correction of a large colon volvulus at Cornell at five months in-foal; there was no prior history of colic before that episode and no other significant medical history disclosed at presentation. Clinical Presentation and Diagnostics: On presentation, the patient was quiet, alert, and responsive but moderately painful. Vital parameters were within normal limits, mucous membranes were dark pink and slightly tacky, and the patient’s abdomen appeared moderately distended. Gastrointestinal sounds were diminished to absent in all quadrants. Sedation was administered, an intravenous catheter was placed, and isotonic crystalloid fluids were administered throughout the duration of the workup. Point-of-care blood work was relatively unremarkable with a packed cell volume (PCV) of 34%, total solids (TS) of 6.4 g/dL, and a lactate of 0.92 mmol/L; it was determined that the patient had no severe metabolic derangements. A rectal examination revealed a gas-distended viscus in the right caudal abdomen, a tight cecal band coursing transversely in the mid-right abdomen, and a palpable nephrosplenic space. Abdominal ultrasound revealed diffusely thickened colon walls of 1.0 – 2.0 cm, with normal thickness reported as 2.0 – 3.75 mm1, large colonic mesenteric vessels against the right body wall, and a small amount of slightly echogenic free peritoneal fluid. Abdominocentesis yielded a stream of lightly serosanguinous peritoneal fluid with a lactate value of 1.01 mmol/L, Page | 3 which was slightly elevated compared to the peripheral value. No net reflux was obtained during nasogastric intubation. Differential Diagnoses: Based on history, signalment, degree of pain, physical exam findings, rectal palpation, and ultrasonography, large colon volvulus was suspected as the most likely differential diagnosis and right dorsal displacement of the large colon remained a possibility. Surgical intervention was discussed, elected, and pursued immediately. Treatment: The mare received perioperative fluid therapy, Gentamicin and K-Penicillin for broadspectrum antimicrobial coverage, and Flunixin meglumine prior to anesthetic induction. The patient was induced under general anesthesia and positioned in dorsal recumbency for an exploratory celiotomy. Upon entering the abdomen, a 360° large colon volvulus entrapping the cecum was identified. The large colon was slightly purple and diffusely edematous with congested mesenteric vasculature, but the large bowel was relatively non-compromised based on mesenteric pulse quality. Using gas decompression and physical manipulation in a clockwise direction, the volvulus was corrected and the colon was replaced into the abdomen in normal anatomic orientation. Based on the viability of the colon, a resection and anastomosis was not considered necessary. Careful examination of the remaining gastrointestinal tract revealed no abnormalities. A colopexy was performed from the ventral band of the left ventral colon to the body wall, approximately 10 cm to the left of midline. The body wall was scored and five cruciate sutures of #2 PDS were pre-placed through the seromuscular layer of the left ventral colon ventral band and the internal rectus fascia of the body wall, which were then brought into Page | 4 apposition by securing each suture. The abdomen was copiously lavaged and the ventral midline incision was closed routinely. The incision site was covered with sterile gauze and an Ioban drape, and a “belly-band,” was secured around the abdomen prior to recovery from anesthesia. Once recovered, the patient was returned to a stall in the intensive care unit; it was decided that the foal would be re-introduced the next morning. Treatment with Polymyxin B had been initiated intra-operatively to combat endotoxemia. The mare received plasma (a natural colloid thought to have anti-endotoxic antibodies2) and a continuous rate infusion of Lidocaine was initiated for its analgesic properties. Isotonic crystalloid fluids (Plasmalyte-A) were supplemented with CaMgPK to support the metabolic demand of lactation and administered at twice maintenance rate. K-Penicillin and Gentamicin were continued for antimicrobial coverage, in addition to an anti-inflammatory dose of Flunixin meglumine. Anti-laminitic therapy consisted of Pentoxifylline and ice boots placed on each of the patient’s limbs. Omeprazole was administered as a gastroprotectant. The mare was milked frequently in preparation of the foal's impending arrival. Overnight, the patient rested comfortably and passed multiple piles of normal to soft manure. Blood work suggested mild dehydration and the fluid rate was adjusted accordingly. The following morning’s physical exam revealed improved gastrointestinal motility compared to presentation. In-house blood work revealed a PCV of 37% and a TS of 5.4 g/dL, suggesting that the patient had some degree of protein loss through the edematous large colon. Inspection of the incision revealed minimal serosanguinous discharge with minimal inflammation; the bandage was replaced and re-secured. Small bran mashes were offered in addition to free choice water, and the mare’s foal was reintroduced without incident. Page | 5 The following day, the mare’s physical exam and blood work were normal, and plasma, Lidocaine, and Polymyxin B were discontinued. Hay was re-introduced slowly. The mare continued to improve daily, and meals were increased in frequency and quantity. Four days after surgery, a Complete Blood Count (CBC) was unremarkable and therefore fluids, antibiotics, and Pentoxifylline were discontinued and the ice boots were removed. The patient’s systemic wellbeing was carefully monitored until discharge six days after surgery. Postoperative discharge instructions included careful inspection of the incision and systemic monitoring for infection, slow re-feeding back to a normal feeding schedule, and initial stall rest followed by restricted exercise over the subsequent three-month period. Follow-up: The patient returned to the Cornell Equine Hospital on 7/13/13 for an incisional infection and substantial weight loss. On visual inspection, there was no evidence of dehiscence or loss of stability of the abdominal sutures. Abdominal ultrasound of the ventral abdomen demonstrated an intact colopexy site and no large fluid pockets deep to the suture line. An aerobic culture of the discharge material was submitted for analysis. A routine dental floating was performed, and the patient was discharged on oral antibiotics (TMS) and instructions to flush the incisional openings and increase feed intake to meet the high-energy demands of lactation and surgical recovery. The mare did well thereafter with anticipated continued use as a broodmare. Discussion: Etiology and presentation of large colon volvulus: Large colon volvulus is a surgical lesion of the gastrointestinal tract thought to be secondary to gas distention of the colon, and represents 17 – 34% of cases requiring exploratory celiotomy3,4. The large colon is susceptible to both displacement and volvulus, as it is freely Page | 6 mobile in the abdomen with only a single mesenteric attachment to the body wall near the base of the cecum. The colon rotates along the longitudinal axis of its mesentery, and depending on the degree of the twist, both venous and arterial circulation can become significantly compromised4. Reported risk factors for large colon volvulus include recent parturition, dietary changes, and access to lush pasture, and broodmares are an over-represented population5. Physical presentation varies based on rapidity of development and progression of a complete volvulus, but the most consistent findings are abdominal distention and intractable abdominal pain. Horses will initially have normal cardiovascular parameters that decompensate over time and rectal palpation findings are variable. The most common direction of volvulus is a dorsomedial movement of the right ventral colon relative to the cecocolic ligament, and most occur at the level of or proximal to the cecocolic ligament, although volvulus can also occur at the level of the sternal and diaphragmatic flexures5. Diagnostic utility during large colon volvulus work-up: Transabdominal ultrasound has been adopted as a standard diagnostic tool during a colic workup to assess the presence and quality of peritoneal fluid, evaluate for gastric distention, examine the content, character, and motility of both the small and large intestine, and evaluate intestinal wall thickness6. It has been documented to facilitate the diagnosis of both large colon displacement and 180° volvulus with high specificity4. Ultrasonographic imaging of colonic vessels coursing laterally on the right side of the abdomen suggests a profoundly increased likelihood of surgical diagnosis of either a right dorsal displacement of 180° volvulus of the large colon in comparison to those cases in which vessels are not visualized. In a normal horse, the colonic vasculature resides in the mesentery along the medial aspect of the colon, and should not be visible on transabdominal ultrasound examination, but if the colon is displaced or twists along Page | 7 the mesenteric axis such that the medial aspect of the colon comes to sit laterally, these vessels can be imaged against the body wall4. This imaging finding has been found to be highly specific and moderately sensitive for the detection of right dorsal displacement or 180° volvulus of the large colon. In the case of a 360° volvulus in which the colon completes a full rotation, mesenteric vasculature is not visualized against the body wall unless imaging is performed directly at the level of the volvulus origin or if the degree of volvulus shifts between time of imaging and surgical diagnosis4. In addition, it has been found that there is diagnostic value in imaging the left ventrum of the abdomen whenever a volvulus is suspected. Visualization of the nonsacculated left dorsal colon in a ventral position is indicative of a 180° or 540° volvulus; in a normal abdomen, ultrasonography of this location should demonstrate sacculated left ventral colon, which is easily distinguishable from nonsacculated bowel. Unfortunately, a 360° degree volvulus may image normally from the left ventral body wall7. Other findings on transabdominal ultrasound that would be consistent with a large colon volvulus include thickened or edematous colon wall, colonic distention with gas and/or ingesta, and diminished or absent colonic motility6. Measurement of both peripheral and peritoneal fluid lactate values has been assessed for diagnostic utility during a colic workup. For those horses with a 360° degree volvulus, a plasma lactate concentration <6 mmol/L at the time of admission yielded >90% chance of survival following surgery, whereas only 30% of those horses with plasma lactate concentration >7 mmol/L at the time of admission survived to discharge. The prognostic value of peripheral lactate as it relates to bowel viability is somewhat debated, though, because it is affected by the degree of systemic hypoperfusion and subsequent organ dysfunction in addition to bowel ischemia8. Elevated peritoneal fluid lactate values have been determined to be more specific to Page | 8 the presence of compromised bowel and are thought to better predict the need for surgery or intestinal resection in comparison to peripheral lactate values9. Surgical correction of large colon volvulus: Upon surgically entering the abdomen and identifying a large colon volvulus, correction and replacement of the large colon may be manually difficult if the colon is particularly full or edematous. Correction is best achieved by manipulating the colon from its base in a clockwise direction, and success is evaluated based on gas translocation and return of normal serosal color. Other indications that a volvulus is relieved include normal position of the cecum and cecocolic ligament, and palpating the mesenteric attachment of the right dorsal colon to the dorsal body wall in the straight line5. Upon replacing the colon in its normal position, the surgeon has several options: no further intervention, euthanasia, large colon resection, and colopexy, the last of which can be combined with an enterotomy if warranted to evacuate a full colon prior to fixation5. Evaluation of colon viability will guide this decision, and, in particular, serosal color, mesenteric arterial pulse quality, and mesenteric and mural edema should be assessed and considered10. Intraoperative markers associated with poor survival include black mucosal color (if assessed during an enterotomy), poor return of perfusion after de-torsion, and rising packed cell volume and falling total solids values during surgery5. There is a 15% recurrence rate for large colon displacement and volvulus, although specific contributing factors have not been identified5; this rate goes up to as high as 80% following two surgical corrections of volvulus, and broodmares appear to be the population at the highest risk for recurrence11. A large colon resection is indicated in cases with full-thickness, mural defects in the large colon. Reports have described resection of 50% to 95% of the large colon, depending on the Page | 9 level of the origin of the volvulus and the amount of remaining viable colon. Lesions distal to the apex of the cecocolic ligament are the most amenable to surgical removal, and successful outcome has been reported in 82% of cases. A twist at the level of the cecocolic ligament may be amenable for resection, depending on the viability of the right dorsal and ventral colons at the proposed site of resection12. End-to-end anastomosis, in which the bowel ends are directly apposed, can be used for resections at least 10 cm from the cecocolic ligament, whereas side-toside anastomoses are preferred following resection of the colon closer to or proximal to the cecocolic ligament in an attempt to reduce tension on the anastamotic site5, and in areas of disparate lumen diameter12. Techniques have been described using hand-suturing or surgical stapling equipment12. In performing a resection, the diseased colon and the associated endotoxic load is removed, thereby potentially increasing chance of survival. The outcome of a resection is more favorable if the line of devitalized bowel is found distal to the cecocolic ligament, but this procedure always carries a high risk of complication, including dehiscence at the anastamotic site, and incurs increased anesthesia time5 and more intensive postoperative care13. Complications secondary to large colon resection include persistent endotoxemia, peritonitis secondary devitalized bowel, postoperative pain, ileus, hemorrhage, diarrhea, and weight loss. Normal stool consistency is typically achieved in five to seven days postoperatively, but these horses will have a lifelong increased water and phosphorous requirement and require a highly digestible diet5. After surviving the immediate postoperative period, longterm complications are relatively uncommon if appropriate dietary adjustments are made12. The overall prognosis following large colon resection depends on the reason for performing the resection; the procedure itself carries inherent risk, and those horses treated with a resection for a non-strangulating lesion have a higher short-term survival rate than those treated with a resection Page | 10 for a strangulating lesion5. In cases in which the colon and/or systemic status of the patient are compromised intra-operatively, healing of the resection site is reported to be poor, and the success rate is less than 50%12. Another surgical option described to prevent recurrence of large colon volvulus is colopexy in which an adhesion is created between the colon and the abdominal wall. Colopexies should be reserved for large colon volvulus cases with relatively healthy large bowel, and should not be performed if the large colon is significantly edematous or compromised10. Suturing an unhealthy colon to the body wall will compromise its ability to survive as the colon may become necrotic, friable, and may tear at the suture sites. In these cases, large colon resection is a better option if marginally viable or nonviable sections of colon are present11. It is recommended that a colopexy be preceded by an enterotomy if the colon is full with ingesta in order to reduce the strain on the colopexy site during recovery; this procedure also allows assessment of mucosal color, which is a good indicator of bowel viability3. Several open techniques of colopexy have been compared; suturing the left colon to the abdominal wall was determined to be the most effective procedure at preventing manual creation of large colon displacement and large colon volvulus. This technique has also been described as being relatively easy to perform in a technical sense, and requiring a short amount of additional surgical time11. A shallow incision is made through the peritoneum about 8-10 cm parallel to the left of the abdominal incision, and retroperitoneal fat is bluntly stripped away to reveal the internal rectus muscle. The ventral or lateral taenia of the left ventral colon, approximately halfway between the sternal flexure and pelvic flexure, is sutured to the body wall, including the entire width of the taenia3. Penetration of the bowel lumen must be avoided during suture placement to prevent leakage of ingesta around the sutures and subsequent peritonitis11. Page | 11 Polypropylene and chromic gut suture materials have been compared for use in colopexies; chromic gut usage resulted in adhesions that varied in formation in duration, whereas polypropylene consistently yielded firm adhesions locally at the site of placement. In the described technique, several interrupted sutures are preplaced and then secured to draw the taenia against the body wall uniformly10. The ideal colopexy suture line length is between 15 – 20 cm3. In addition, a laparoscopic colopexy technique has been described; it is minimally invasive and can be used as a delayed procedure allowing a compromised colon time to heal following correction of volvulus3. Postoperative considerations in the large colon volvulus patient: Reported complications following a colopexy include intermittent abdominal pain, dehiscence of the colopexy site and need for reoperation, subcutaneous fistula tracts, delayed passage of ingesta11, weight loss14, and catastrophic colon rupture, which has been described in association with a cachectic state in a select case3. Subcutaneous fistula tracts were described as a direct result of bowel lumen penetration upon placement of the colopexy suture3. Delayed passage of ingesta is thought to be secondary to increased stabilization of the colon and could theoretically predispose to impaction, although this has not been observed clinically11. Cecal tympany has occasionally been seen in cases in which the colopexy site has been placed too close to the sternal flexure, placing tension on the cecocolic ligament 3. Fatality rate attributed directly to complications of the colopexy procedure is about 6.8%10. Historically, the colopexy procedure has been reserved for nonperformance animals5. This procedure has been avoided in high-level performance horses due to the unknown effect of colopexy at high speeds and under high levels of mechanical stress11. Several clinical cases of colopexy have been followed long-term, including patients of varying signalments fulfilling Page | 12 careers as broodmares, pleasure riding horses, and one report of a successful show hunter11. The described cases included those patients ranging from first to third correction of large colon volvulus, and in all patients normal body weight was achieved and there were no postoperative episodes of abdominal pain. In addition, colopexy has been performed in pregnant mares that have survived and delivered a live, healthy foal. It has been shown that broodmares undergoing colopexy can be bred back in a timely manner, have normal pregnancies, and can deliver in a normal fashion following the procedure11. There is some concern that foals from mares with colopexy have increased incidence and severity of angular limb deformities, but this claim has not been substantiated3. Colopexies can be performed at the first surgery for large colon volvulus in young to middle-aged broodmares because of the high risk of recurrence so early in the anticipated career3. Overall, the consensus for the best surgical method to prevent the recurrence of large colon volvulus is highly case- and surgeon-dependent and a definitive plan should not be elected prior to comprehensive evaluation of the large colon at surgery. Strangulating large colon volvulus (greater than or equal to 360°) has reported survival rates to discharge ranging between 36 and 83%2,15. The variables most significantly associated with reduced long-term survival include abnormal serosal color of the large colon intraoperatively, postoperative tachycardia, and colic during postoperative hospitalization. A change in serosal color is indicative of vascular compromise, which may correlate with the degree of the systemic inflammatory response as a result of a loss of mucosal barrier function and transmural migration of microbes and endotoxin into the peritoneum and circulation. Persistent tachycardia postoperatively is associated with the degree of systemic inflammatory response secondary to endotoxemia. Colic may be the result of ischemia, adhesion formation, or stenosis, none of which carries a favorable prognosis15. Page | 13 All horses undergoing surgical correction of large colon volvulus are at risk for postoperative complications including severe endotoxemia that can precede multiple organ dysfunction syndrome (MODS), continued ischemic necrosis of the large colon, hypoproteinemia, and diarrhea2. Postoperative monitoring should focus on attitude, appetite, abdominal pain and distention, fecal production and consistency, urination, vital parameters, borborygmi, oral mucous membrane color and moisture, and capillary refill time every few hours in order to asses for clinical signs of the aforementioned complications2. PCV and TS should also be monitored frequently for the first 24 to 72 hours after surgery2. Changes in TS should mirror changes in PCV unless hemorrhage or protein loss occurs; a fall in total solids is suggestive of a loss of bowel mucosal integrity secondary to ischemia following a strangulating large colon obstruction, or diarrhea. An increase in PCV with a concurrent decrease in TS is often associated with endotoxemia (the hemodynamic, hematologic, and metabolic effects of which are well documented in the horse), and this particular laboratory data pattern carries a poor prognosis2,16,17. Page | 14 References: 1 Hendrickson EHS, Malone ED, Sage AM. Identification of normal parameters for ultrasonographic examination of the equine large colon and cecum. Can Vet J 2007;48:289–291. 2 Southwood, LL. Postoperative management of the large colon volvulus patient. Vet Clin Equine 2004;20:167–197. 3 Hance, SR. Colopexy. Vet Clin North Am Equine Pract 1997 Aug;13(2):351–358 . 4 Ness, SL et al. Ultrasonographic visualization of colonic mesenteric vasculature as an indicator of large colon right dorsal displacement or 180° volvulus (or both) in horses. Can Vet J 2012;53: 378-382. 5 Auer JA, Stick JA. Large Intestine. In: Equine Surgery. 4th ed. St. Louis, Missouri: Elsevier Saunders, 2012;454–494. 6 Beccati, MP et al. Is there a statistical correlation between ultrasonographic findings and a definitive diagnosis in horses with acute abdominal pain? Equine Vet J 2011;43(Suppl. 39):98– 105. 7 Abutarbush, SM. Use of ultrasonography to diagnose large colon volvulus in horses. J Am Vet Med Assoc 2006;228(3):409–413. 8 Johnston, K. et al. Plasma Lactate as a Predictor of Colonic Viability and Survival After 360° Volvulus of the Ascending Colon in Horses. Vet Surg 2007;36:563–567. 9 Latson, KM et al. Peritoneal fluid lactate as a marker of intestinal ischaemia in equine colic. Equine vet J 2005;37(4):342–346. 10 Hance SR and Embertson RM. Colopexy in broodmares: 44 cases (1986-1990). J Am Vet Med Assoc 1992;201(5):782–787. 11 Markel, MD. Prevention of Large Colon Displacements and Volvulus. Vet Clin North Am Equine Pract 1989 Aug;5(2):395–405. 12 Bertone, AL. Large Colon Resection. Vet Clin North Am Equine Pract 1989 Aug;5(2):395– 405. 13 Hughes FE and Slone DE. Large Colon Resection. Vet Clin North Am Equine Pract 1997 Aug;13(2):351–358. 14 Markel MD, Dreyfuss DJ, Meagher DM. Colopexy of the equine large colon: comparison of two techniques. J Am Vet Med Assoc 1988;192(3):354–357. Page | 15 15 Suthers, JA. Survival or horses following strangulating large colon volvulus. Equine Vet J 2013;45: 219–223. 16 Fischer, AT. Intensive Care of the Patient After Abdominal Surgery. Vet Clin North Am Equine Pract 1988 Apr;4(1):105–113. 17 Moore, JN. Recognition and Treatment of Endotoxemia. Vet Clin North Am Equine Pract 1988 Apr;4(1):105–113. Page | 16