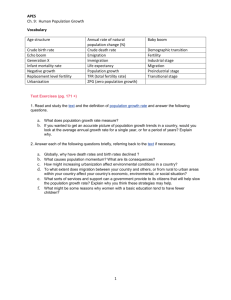
Family Planning Commodity Projection for 2014
advertisement

Family Planning Commodity Projection for 2014-2021 National Institute of Population Research and Training (NIPORT) Conducted by Center for Development Studies Lorna Office Complex (1st floor) 94/A New Eskaton Road August 2013 1 Director General National Institute of Population Research & Training (NIPORT) Ministry of Health and Family Welfare Dhaka Foreword The National Institute of Population Research and Training (NIPORT) has been providing information support to the national family planning program of the MOHFW by conducting studies on different issues relevant to achievement of targets under the family planning program initiated by the Government of the People’s Republic of Bangladesh. As the program continues to expand, flourish and consolidate, it needs, in the process, to look at the demand that program has to meet over a longtime perspective in terms of family planning commodities which are essential for ensuring success. A study to make projections on family planning commodity requirements from 2014-2021 was therefore in order. This exercise, therefore, is an attempt to provide the government, as well as the policy planners, with precise family planning commodity requirements in order to help them work out a road map for the program from 2014 through 2021. I firmly believe, the recommendations put forward in the study would be useful guidelines for the program planners to plan out the future needs with immaculate precision and result. We thank the Center for Development Studies for their excellent job done. We appreciate their sincerity and commitment. Shelina Afroza, PhD 2 Director (Research) National Institute of Population Research & Training (NIPORT) Ministry of Health and Family Welfare Dhaka Preface We are happy to note that the study entitled: Family Planning Commodity Projections for 20142021—has been successfully completed with sincere effort put in by the Center for Development Studies, Dhaka. This is, indeed, something that NIPORT always appreciates. This study is a part of NIPORT’s continuous effort to provide the policy planners and decisionmakers with appropriate knowledge, information and necessary data to enable them to be abreast of actual situation at the field and thus design the program based on that. We believe, the findings and recommendations made under this study will be another milestone in that regard in feeding them with appropriate knowledge and information which they would find useful for application. We appreciate the Center for Development Studies for their excellent work. We hope, they would continue to maintain the same standard and excellence in conducting similar studies in the event they are given the responsibility. Finally, I would like to appreciate the NIPORT team, too, for their persistent effort and hard work in facilitating conduct of the study. (Md Rafiqul Islam Sarker) 3 Acknowledgement The Management of the Center for Development Studies acknowledges, with deep sense of gratitude, the opportunity that NIPORT has given to CDS for being part of this important work accomplished for the interest of the program in the population sector. The Director General, Director Research, and the Evaluation Specialist and Deputy Program Manager, as well as all other officials, staff and personnel of the NIPORT family extended valuable support and cooperation that CDS needed in getting the task completed within the stipulated timeframe. The Core Study Team demonstrated the highest sense of responsibility in accomplishing the task with immaculate precision and correctness warrants special appreciation. All of them maintained strict time-schedule for the discussion meeting called for sharing the views and making the analysis of the materials, data and information collected for the task. We thank all of them. The support staffs were also alert for extending every support the CST needed for the task. They even worked beyond normal office hours with smiling faces, taking it as a challenge to beat the clock under exigency. Finally, it is the concerted effort of all the people involved in the process that required extreme level of determination and commitment. We owe them a lot for what we obtained through their sincere support beyond our expectation. May Almighty Allah bless them and us all. Iftekhar Uddin Ahmed Chairman Center for Development Studies 4 Contents Foreword Preface Acknowledgement Abbreviations Executive Summary 2 3 4 6 7 Chapter 1 1.1 1.2 1.3 1.4 1.5 1.6 1.7 1.8 Introduction Background Rationale Objectives of the Study Scope of Services Methodology Scenarios of Projection Data Projection of Scenarios and Baseline Input Data Data Collection Chapter 2 2.1 2.2 Findings Introduction Projected number of users and acceptors according to scenario-I Projected family planning commodities requirements according to scenario-I Projected number of method users and acceptors according to Scenario-II Projected family planning commodity requirements according to Scenario-II Projected number of method users and acceptors according to scenario-III Projected family planning commodities requirements according to scenario-III Projected number of method users and acceptors according to scenario-IV Projected family planning commodities requirements according to scenario-IV Conclusion and Policy Implications Introduction Reaching Unmet Need for Contraception for Limiters and Spacers Transforming Intenders into Users Shifting Traditional Method toward Modern Methods Achieve TFR= 1.7 per woman Formulating the Quality Strategy Policy Implications Limitations Recommendations 2.3 2.4 2.5 2.6 2.7 2.8 2.9 Chapter 3 3.1 3.2 3.3 3.4 3.5 3.6 3.7 3.8 3.9 Bibliography Appendix-A/B Research Team 11 12 12 13 13 19 20 23 25 25 28 29 31 33 34 36 37 38 38 38 39 39 39 40 40 40 42 44/48 54 5 Abbreviations BBS Bangladesh Bureau of Statistics BDHS Bangladesh Demographic and Health Survey CPR Contraceptive Prevalence Rate CYP Couple Year Protection DDS Drugs and Dietary Supplements DGFP Directorate General of Family Planning FP Family Planning GoB Government of Bangladesh HPNSDP Health, Population and Nutrition Sector Development Program IP Infection Prevention IUD Intrauterine Device LAPM Long Acting Permanent Method LA/PM Long Acting/ Permanent Method LMIS Logistics Management Information System MIS Management Information System MOHFW Ministry of Health and Family Welfare MWRA Married Women of Reproductive Age NGO Non-Government Organization NIPORT National Institute of Population Research and Training OP Operation Plan RH Reproductive health TFR Total Fertility Rate UNFPA United Nations Population Fund WHO World Health Organization WRA Women of Reproductive Age 6 EXECUTIVE SUMMARY Traditionally, family planning program plans contain specific targets. A demographic target, in terms of fertility rates is set first for a specified year in the future. Based on this target, required numbers of acceptors1 and users2 are projected under different assumptions. Target-setting by planners without consideration for the needs of the clients, most of whom are women, often leads to unsatisfactory and inefficient use of contraceptives. The clients and potential clients are those couples who intend to use family planning services to limit the total number of children they would like to have and to space those children. The family planning program should provide them with appropriate contraceptives that fit their specific needs. A related issue is the quality of services, which, reportedly being unsatisfactory, is ‘often the reason why couples are not using family planning services even when they have the need, or are not using a method that is appropriate for them'. A client-oriented approach would focus on ways to: (l) expand the program to serve couples who intend to use family planning services' and (2) improve the quality of services so that more clients will use appropriate methods correctly and longer. The purpose of this exercise is to project the contraceptive commodity requirements keeping in mind the vision of the family planning program. The objectives of the exercise are to: Outline the vision of reproductive health and family planning in the future; Identify strategies, under different scenarios, to achieve reproductive health and family planning goals; and Develop specific recommendations for utilization of effective strategies to achieve Program goals The projection for strategic planning was derived by using the microcomputer-based FamPlan system of models. A total of four sets of projections and associated contraceptive commodity requirements were made using the FamPlan model. The FamPlan system of models is designed to help development planners to transform their population policies into implementation and operational plans. It is also aimed at helping family planning managers to estimate contraceptive commodity requirements and to allocate resources effectively among different family planning delivery systems. The different scenarios generated in this study include: Develop year-wise Family Planning Commodity Projections for 2014-2021 in Bangladesh assuming that all unmet need for family planning will be satisfied by 2016 as specified in the HPNSDP, and it should also be based on the medium variant projections of the United Nations Population Division projections that assume a more gradual contraceptive prevalence increase based on historical trends; Develop year-wise projections of contraceptive commodities for 2014-2021 considering three key factors: a) growth in the numbers of women of reproductive age as a consequence of high fertility rates in the past; b) increasing demand for family planning; and, c) changes in the family planning methods used, particularly the shift from traditional to modern methods as programs mature; 1 Acceptors are the number of new users required to achieve the specified growth in total users (users next year minus users this year) plus the number of new users required to replace those that discontinue use, age out of the age group, or die, minus the number of current users aging into the age group. 2 Users: The number of women who are using some form of contraception. 7 Develop year-wise family planning commodity projection for 2014-2021 on the assumption that the private sector provides an important share of family planning services in Bangladesh; Assess the complete family planning commodity projection for 2014-2021 status on the basis of Demographic Pressures: More Couples of Reproductive Age, Increasing Demand for Contraceptives, Contraceptive Users and Method Mix; Comparative pictures of all scenarios indicate which one is most effective and which one is less effective. Among the scenarios generated, the most effective scenario is achieving unmet need of family planning and the less effective is the elimination of traditional methods. Given the situation, this suggests that there is a scope for increasing CPR. If unmet need can be reduced at all stages, then it will have significant impact on the commodity requirements as well as reaching demographic goals by 2016. Second set of projection for the contraceptive requirements is made under the assumption that the replacement fertility will be achieved by 2016. For instance, under the assumption of eliminating unmet need for poor contraception, the acceptors will be almost doubled between 2014 and 2021. Long acting methods like IUD is also effective for a country like Bangladesh. It has demonstrative effect on the achievement of fertility and consequently on contraceptive commodity requirements. However, to implement IUD quality services need to be ensured along with side-effect management. It is important to mention here that in rural Bangladesh RTI is high among the IUD users. Therefore, management of RTI and counseling to mothers are important determinants of IUD use. Considering that, couples who do not want any more children should be segmented for IUD use. One of the problems of male and female sterilization users is that by the time they come to accept sterilization, they have already achieved desired fertility, and thus leave little demographic impact, excepting the fact that the increased use of these methods reduces the burden of other modern methods, such as pill and condom, and in the long run commodity requirements will become lower and the program will be cost-effective to some extent. What will be contraceptive commodity requirements if the male sterilization can be increased? Projected information shows that there will be fewer users than it would be required under the other assumptions. The increased use of male sterilization has significant effect on the achievement of replacement fertility, because relatively lower CPR would be required to meet the demographic goal. Under this assumption, there will be less requirement of pill and increased requirement of male sterilizations. If this could be done, then the program will be sustainable and in the long run it will be more cost-effective. Future Strategies to achieve Demographic Objectives: The family planning program should provide acceptors and users with appropriate contraceptives that fit their specific needs. A related issue is the quality of services. A common reason why couples do not use family planning services even when they need them, or are not using the method best suited to them, is unsatisfactory quality of services. The quality of services can be ensured through regular visits of the households and management of side-effects when they need them. About 50 percent users of pill discontinue within one year. Discontinuation is the highest for condom users with only third clients continuing up to one year; discontinuation for IUD users is 35 percent indicating that IUD use would be more crucial to achieving demographic target. Fear of side-effect is a major reason for non-use. Side-effect management services are not welldeveloped. There is an inadequate monitoring and supervision system. A client-oriented approach would focus on ways to improve the quality of services so that more clients will use appropriate methods correctly and longer. 8 Raising continuation Rates and improving use-Effectiveness: The current rates of continuation and use-effectiveness are less satisfactory than the desired level. If the program is to achieve its demographic goals, all possible efforts should be directed toward enhancing these rates. Strategically, this implies improved quality of care and services. A coordinated set of health and family planning services would be necessary to implement the quality strategy. The following issues need to be addressed for any improvement in the quality of care and services: Identifying, monitoring, and providing treatment of side-effects and complications strengthening the chain of supervision for ensuring side-effect management. It is assumed that improvements in the quality of care and services and realization of the expectations of the current intenders will result in a shift in the contraceptive method mix toward longer-acting methods. Currently, the family planning program favors the modern, reversible methods. Some of the important issues regarding low use of longer-term methods are: lack of adequate and hygienic service facilities for inserting and removing IUDs; noncompliance with minimum aseptic measures (e.g., washing hands before examination, using sterilized gloves, etc.), noncompliance with the standard technical procedures (e.g., taking weight, measuring blood pressure, enquiring about pelvic bleeding, performing pelvic examination, etc.); lack of appropriate brands of IUDs with fewer side-effects and complications; Although fertility in Bangladesh has been declining, it is not, however, enough to reduce population growth because of population momentum which is due to high fertility in the past. The proportion under 15 is high, and as a result of the young age structure of the population, the population will continue to grow for several decades even if we achieve replacement fertility as targeted. Delay in age at marriage, increasing the age at first birth, spacing of births and widely dispersed births may reduce population momentum. Therefore, accessibility of contraceptives is crucial to the newly married couples and adolescents to accelerate the demographic transition. Program should also ensure uninterrupted contraceptive supplies to them and it should get appropriate emphasis in the program, such as providing an uninterrupted supply of contraceptive commensurate with needs, more trained manpower within logistics management system, etc. The training, either formal or informal, should continue, as it helps increase the knowledge and skill of the personnel, especially the storekeepers at the warehouses, which is consistently related to achieving the effective contraceptive distribution. 9 CHAPTER 01 INTRODUCTION 1. Background The Government has developed the National Population Policy which seeks to reduce fertility to replacement level by 2015. This requires a further TFR decline of 0.3 children per couple compared to current TFR 2.3 children per couple (BDHS 2011). But, even at replacement fertility, the country will be adding two million annually to the population due to high fertility in the past, and many in the population field feel that the decline needs to be greater, with a target of 1.0 below present fertility (i.e. to TFR 1.7), projected to have substantial benefits across many sectors. It will not fall any lower, so all future population growth will be determined entirely by the fertility level. High rate of population growth and the resultant increase in population size impede the process of achieving the objectives in various sectors of the economy. Therefore, those ministries and agencies whose target population is affected by population growth would have to share the burden of responsibility of population control and family planning, in addition to the targeted interventions of MOHFW. The development issues relating to the population of Bangladesh are convincing the families of the need and benefits of delayed marriage for their daughters; newly-wed couples should wait before having their first child, especially if the bride is young; small and medium scale employment opportunities for young women be generated in rural areas, so that marriage does not have to follow so closely on school drop-out; high school drop-out rates be reduced; services can be designed to more effectively educate unmarried adolescents on reproduction, and alternative options to early marriage. A social movement to eliminate dowry needs to be encouraged and supported. All these challenges are to be addressed through the interventions of other relevant ministries, in addition to the interventions within MOHFW’s jurisdiction. The Family Planning (FP) Program has built a nationwide community-based FP service delivery system, relying primarily on non-clinical methods such as oral pills and condoms. The current pattern of temporary contraceptive use, with oral pill users being close to 30% of all married couples, is reaching saturation (only two other developing countries exceed this proportion), but other individual methods do not even account for 10% each. With persistent early marriage and high fertility, many women have completed their childbearing by the mid late twenties, leaving them with two decades of reproductive life to avoid unwanted pregnancies. However, the proportions of couples relying on long-acting or permanent FP methods (IUD, implants, male or female sterilization) remains very low (less than 15%). Diversified and mass-scale FP services will need to be undertaken to bring back the tempo of 1980s and achieve the target of fertility to replacement level. As per BDHS report-2011, CPR is 61.2% and TFR is 2.3 which were respectively 55.8% and 2.7 in 2007 (BDHS-07). Under the HPNSDP, CPR and TFR having been targeted as 72% and 2.00 /women respectively by the year 2016, the following strategies will be pursued to achieve the targets: (i) Increasing the contribution of long-acting and permanent methods to the method mix; (ii) Reducing the unmet need from 17.1% (BDHS-07) to 9%; (iii) Ensuring uninterrupted supply of logistics; (iv) Implementing special interventions/programs for the low-performing and hard-to-reach areas; and (v) Massive awareness development program. 10 On the other hand, unmet need for Family Planning was 14% (BDHS-11). The reasons for higher unmet need were as follows: (i) Stock-out of contraceptives at the field level; (ii) Shortage of manpower at the field level: (iii) Below par monitoring and supervision; (iv) Inadequate program interventions for the low-performing and hard-to-reach areas. During the last few years, required numbers of manpower were recruited and contraceptives forecasting and procurement had been made time-bound. Special activities were undertaken to ensure effective monitoring and supervision at all levels. In addition, considering the initiatives taken so far, and the program interventions made under various OPs of DGFP for the HPNSDP, it will be possible to reduce the unmet need to 9% in 2016 from 17.1 % (2007). The demand for family planning services is defined as the sum total of unmet need and total contraceptive use. The 2011 BDHS shows that demand for family planning services is 75 percent and proportion of demand satisfied (total contraceptive use divided by the sum of total unmet and total contraceptive use) is 82 percent (BDHS: 2011). The Health Population Nutrition Sector Development Program (HPNSDP) has set a target of reducing unmet need for family planning services to 9 percent by 2016 (BDHS 2011). 1.2 Rationale Good reproductive health programs depend on a reliable supply of certain essential commodities. When supplies are inadequate, or are interrupted, even well-planned interventions may falter and opportunities may be lost. The importance of these essential items comes into sharp focus when supply shortages, or stock-outs, occur. Nationally, progress towards family planning goals is now measured by tracking the number of additional users of family planning. To accomplish the tasks defined and get the program going from the present level of attainment to targeted attainment, there needs to be made comprehensive and trend-based projections on the commodity that the program will need through 2014-2021 in order that the program implementation does not suffer from any shortcomings and lack of supply and support essentially needed for targeted achievements. The commodity projection will help, using the number of additional users as the indicator, to measure progress in family planning interventions. The proposed study is designed to make that projections based on various assumptions with the target to achieve the following objectives: 1.3 Objectives of the study The broad objective of this exercise is to assess the future needs for contraceptive commodities through projecting Family Planning Commodity Projection for 2014-2021 in Bangladesh under different assumptions. The specific objectives of the study are to: i. Develop year-wise Family Planning Commodity Projections for 2014-2021 in Bangladesh assuming that all unmet need for family planning will be satisfied by 2016 as specified in the HPNSDP, and it should also be based on the medium variant projections of the United Nations Population Division-projections that assume a more gradual contraceptive prevalence increase that is based on historical trends; ii. Develop year-wise projections of contraceptive commodities for 2014-2021 considering three key factors: a) growth in the numbers of women of reproductive age as a consequence of high fertility rates in the past; b) increasing demand for family 11 planning; and, c) changes in the family planning methods used, particularly the shift from traditional to modern methods as programs mature; iii. Develop year-wise family planning commodity projection for 2014-2021 on the assumption that the private sector provides an important share of family planning services in Bangladesh; iv. Assess the complete family planning commodity projection for 2014-2021 status on the basis of Demographic Pressures: More Couples of Reproductive Age, Increasing Demand for Contraceptives, Contraceptive Users and Method Mix; v. Generate a set of recommendations for implementation of the year-wise family planning commodity projections in Bangladesh in consultation with different stakeholders including Directorate of Family Planning. 1.4 Scope of services Commodity needs are projected according to population data, contraceptive prevalence trends, anticipated changes in the contraceptive method mix, and average annual supply costs per method. Bangladesh Demographic Health Survey 2011 data have been used to make estimates and projections for numbers of women aged 15-49 and total fertility rates (TFRs). Standard UN procedure has been used to create a schedule of the family planning commodity projection. The procedure of the projections has been defined. The projection results have been shared with different stakeholders including Logistics Unit of Family Planning Directorate under guidance of NIPORT before finalization of the report. 1.5 Methodology 1.5.1 Family Planning Commodity Projection Ideally, quantification for projection is an activity that includes constant monitoring of inventory levels, product consumption rates, and other information—including programmatic and environmental factors— that may affect future demand. If the logistics management information system (LMIS) is designed well and kept up-to-date, the staff responsible for quantification and procurement will have with them all the consumption and stock level information they need. While consumption data is considered as the gold standard for contraceptive projection, such data are not always accurate, reliable, or readily available. Below are the descriptions of the product characteristics and special projection considerations for the different types of family planning methods; different types of data to be used for projecting family planning commodity supplies; and the steps in the projection methodology, including guidance on how to adjust for problems with data quality and how to analyze the validity of different projections. 1.5.2 Projection Considerations When projecting for short-acting contraceptive methods, we have considered the following product characteristics: Oral contraceptive pills For non-emergency oral contraceptives, two types are usually available: combined oral contraceptives (COCs-the most popular), and progestin-only oral contraceptives (POCs). Women who cannot take products that contain levonorgestrel (due to side-effects), or lactating women, can take progestin-only oral contraceptives. The number of users of combined orals in 12 any situation almost always exceeds the number of users of progestin-only orals. In addition, many service providers do not have clear guidelines about how to counsel women who might be eligible to use progestin-only orals—this makes it more difficult to accurately estimate the demand for POCs. Injectables Injectables are available in one-month, two-month, and three-month forms (i.e., a woman receives an injection once a month, every two months, or every three months). The most popular is the three-month injectables. When projecting for injectables, included in the forecast are syringes and the correct size needles. Condoms Male and female condoms are barrier devices that are used during sexual intercourse to prevent pregnancy and reduce the transmission of the human immunodeficiency virus (HIV) and sexually transmitted infections (STIs). Male condoms are inexpensive and easy to use, with few sideeffects (usually an allergic reaction to latex). It does not require a visit to a clinic or a medical prescription; public sector health programs often offer them for free or at nominal price. The use of the male condom depends on the initiative and motivation of individual men. Use of the female condom, while controlled by women, requires practice to learn how to use correctly and has a significantly higher per unit cost. The female condom has few, if any, sideeffects, and current evidence indicates that it can be reused after washing, disinfection, and relubrication. Using it in our FP Program is still a long way off. E m e r g e n c y c o n t r a c e p t i ve p i l l The emergency contraceptive pill (ECP), provided in a one-pill or two-pill pack, has a high dose of the same hormones used in non-emergency oral contraceptives (the number of pills depends on the brand). ECP can be either combination or progestin-only pills. The population that uses these products is a sub-set of the total population interested in using a modern method of contraception. For example, if a woman is using a condom and it breaks, if she forgets to take her pill, or if she receives her injection late, she would know immediately that her short-acting method had failed. If she knew about ECP, she could use it as a back-up method. However, a woman using LA/PM would not necessarily know immediately if her method had failed; therefore, users of LA/PM are less likely to use ECP. C yc l e b e a d s Cycle beads are based on the standard-days-method, a non-hormonal method of contraception that relies on fertility awareness (knowing the days of her menstrual cycle when a woman is most likely to become pregnant— on those days, she either avoids sex or uses a backup method). Cycle beads are often recommended for women who either do not wish to or are unable to use hormonal or barrier methods of contraception. Users of cycle beads usually (1) have a religious/moral objection to barrier, hormonal, or permanent methods; (2) are interested in modern methods but may have experienced side-effects; or (3) may not have regular access to services. However, because some women may use a backup method during the days when they are most likely to conceive, the use of cycle beads may overlap with other methods. As with any new method, it is important to train providers to counsel women on the appropriate use of cycle beads; they are not appropriate for all women (women whose cycles are irregular or are outside the 26–32-day range). Likewise, to establish the size of the potential user population, determine if only certain service providers will carry cycle beads and the locations of the SDPs. It is unlikely that a woman already using a modern method of contraception would 13 switch to cycle beads, so new users of cycle beads are likely to be those who are using traditional methods or no method. Cycle beads do not have an expiry date; however, a small rubber ring that accompanies the beads may wear out after a few years and, over time, the calendars inside the packages may become outdated. For Long-Acting and Permanent Methods of Contraception, intrauterine devices [IUDs], hormonal implants, female and male sterilization have been considered. It has lagged behind for several reasons, despite their high effectiveness and popularity with users. For several reasons, contraceptive supplies for Long-Acting and Permanent Methods (LA/PM) are more complicated to forecast than short-acting methods. For implants and IUDs, in addition to the device itself, additional products are required for both insertion and removal. Female and male sterilization requires special clinical training, administration of anesthesia, and use of drugs for pain management. All LA/PM require infection prevention equipment and supplies for health worker protection and for decontamination and sterilization of instruments. Projection of LA/PM will require special consideration. In general, when projecting for LA/PM, the projection will include the estimated quantity of the contraceptive device (IUD, hormonal implant) plus the quantities of reusable instruments, disposable instruments and expendable medical supplies; and, for female and male sterilization, anesthesia drugs and supplies, and pain management drugs. The following product characteristics will be considered when projecting supplies for the LA/PM of contraception: Hormonal implants Hormone-containing contraceptive implants are a highly effective, long-acting, and immediately reversible method of contraception. The implant is inserted under the skin in a woman’s upper arm and remains effective for three to five years, depending on the implant used. Hormonal implants have a small, flexible plastic rod, about the size of a matchstick that releases a progestin hormone. Three types of implants are currently available: Jadelle, a two-rod implant with 75 milligrams (mg) of levonorgestrel in each rod, with a use life of five years Implanon, a one-rod implant with 68 mg of etonogestrel, with a use life of three years Sino-implant II, a lower cost, two-rod implants with 75 mg of levonorgestrel in each rod, with a use life of four years; provided with a disposable trocar. Insertion and removal of implants require a minor surgical procedure. Providers require specific training on insertion, removal, counseling, management of side-effects, infection control procedures, disinfection or sterilization of medical instruments, and disposal of sharp and contaminated wastes. To safely and effectively provide the method, all required equipment, medical instruments, expendable medical supplies, infection prevention, and disinfection/sterilization supplies must be available. These supplies are not packaged in a self-contained kit; therefore, forecast will be made separately for procurement. I n t r a ut e ri n e d e vi c e To prevent pregnancy, a trained provider inserts the IUD, a small, flexible plastic frame, into a woman’s uterus. An IUD is a long-acting, safe, and effective contraceptive method that is quickly reversed by removing the device. The most commonly offered IUDs include the copper T 14 intrauterine device (TCu)-380A and the Multiload-375; both copper bearing IUDs can be used for 12 years or more; and the hormonal IUD—the levonorgestrel-releasing intrauterine system (LNGIUS)—effective for at least five years. A specific set of sterile medical instruments and expendable medical supplies are required for both insertion and removal of an IUD. Sterilization Female and male sterilization are surgical procedures that provide permanent, lifelong protection against pregnancy, and is therefore an option for men and women who do not want more children. Sterilization, one of the most effective contraceptive methods, has a low failure rate, depending on the surgical technique used. In resource-constrained settings, the surgical techniques used most often are mini-laparotomy for women and non-scalpel vasectomy for men. Because sterilization is permanent, it is critical for the client to receive counseling and to give informed consent. Both procedures are non-invasive, relatively simple surgeries, but they must be performed by a specially trained provider (usually a physician or nurse-midwife). A mini-laparotomy must be performed under partial anesthesia, as an incision is made into the abdomen to lift out the fallopian tubes, which are cut and tied, or cauterized. Vasectomy, which only requires local anesthesia, is performed through a small incision in the scrotum where the vas deferens are located, cut and tied, or cauterized. For vasectomy, the procedure is not fully effective for three months; during this time, the couple must use condoms or another contraceptive method. Both mini-laparotomy and vasectomy require specific medical equipment and instruments, and many expendable medical supplies, anesthesia drugs and supplies, and pain management drugs, as well as supplies for infection prevention and disinfection/sterilization of reusable instruments. See appendix C for a list of the products required. 1.5.2. Medical instruments and supplies, drugs, and infection prevention supplies Cont racept i ve devi ces, di sposabl e i nst rument s, and expendabl e medi cal suppl i es While estimating the number of procedures to be performed, the following will be considered: For each product that is inserted or only used once, the quantity needed will be calculated on a direct one-to-one ratio (1:1) to the number of insertions, removals, or surgical sterilization procedures. When more than one unit of the product is needed for each procedure (e.g., sterile gauze pads, surgical drapes), the standard quantity of each product needed will be multiplied, per procedure, by the estimated number of procedures. It will not be possible to use historical consumption data on products with multiple uses for projection of LA/PM, unless the product is used exclusively for projecting the specific LA/PM, or the quantities used for LA/PM are reported separately. Infection prevention (IP) supplies are typically among the expendable supplies purchased and made available for general, multi-purpose use by health facility staff. While a specific quantity of infection prevention items required per procedure is estimated, (e.g., disposable 15 gloves or disinfectant solution), these products may not be used exclusively for LA/PM—unless they are part of a pre-packaged, sterile IUD, implant, or surgical kit. Reusabl e medi cal inst rument s Certain reusable medical instruments are required for insertion and removal of IUDs and implants, and for performing female and male surgical sterilization via mini-laparotomy and non-scalpel vasectomy. Regardless of the type of data used, the forecaster will — Determine whether the reusable instruments are already available and will be used exclusively for LA/PM, or if the instruments are routinely used for other types of procedures. If these reusable instruments have multiple uses, that may affect their availability for LA/PM. Consider the level and type of facility where the method is being provided. For example, mini-laparotomy kits for use in mobile units will contain all medical instruments and supplies required for one procedure, but the availability of the same medical instruments at a district hospital may affect whether the method can be provided or not. Include the expendable medical supplies for disinfection and/or sterilization of reusable instruments, as well as supplies of personal protective equipment (PPE) for health workers (e.g., exam gloves, masks), based on the estimated number of procedures that will be performed. Anest hesi a drugs a nd suppl i es, and pai n management drugs Drugs and supplies are required for female and male surgical sterilization (usually a minilaparotomy and non-scalpel vasectomy). When projecting for these products, it will be ensured that— The quantities of local anesthesia drugs and supplies, distilled water for dilution, and pain management drugs required for each surgical sterilization procedure are standardized for each procedure and should include the dosage form, strength, and dosing schedule for each type of pain management drug. (The correct use of these products should be documented in the clinical protocols for each LA/PM). Ensure that clinical protocols for LA/PM are current and that they specify the drug products and drug combinations, and how they should be administered for pain management during a mini-laparotomy and non-scalpel vasectomy. Alternative combinations and dosages of pain management drugs will also be forecast if the percentage of clients that will be prescribed with one, or the other, combination of drugs can be estimated. Some clients may not be able to tolerate the pain management drugs as set out in the clinical protocols because of allergies, side-effects, or other sensitivities. Other clients may require higher dosages, or more frequent dosing, if they have a low pain threshold. If the number 16 of cases requiring alternative combinations and dosages of pain management drugs represents a significant percentage of the total number of procedures performed, then these cases may be forecast separately. Kits If procuring and supplying contraceptive devices in kits that include all the disposable instruments and expendable medical supplies required for insertion or removal of IUDs or implants, or for performing mini-laparotomy or no-scalpel vasectomy, there will be no need to forecast for these supplies separately, if— quantities supplied in the kit are sufficient to perform one procedure correctly supplies in the kit are used exclusively for the designated LA/PM procedure. 1.6 Sources of Projection Data Census and Survey Data Three types of data can be used for projecting the consumption of contraceptive supplies: consumption data, services data, and demographic data. We consider program targets expressed as a projected number of people to be served. Census 2011 data used for projecting target people and national survey (Bangladesh Demographic and Health Survey) morbidity data used for projection commodities. We used the different types of data to prepare separate forecasts of the estimated consumption for each product. Then, we compared the results of the different forecasts and reconciled them to determine the final estimate of consumption for each product, which we then used as the starting point for projecting quantity. Other sources of data (Consumption Data) Consumption data are historical data on the actual quantities of products dispensed to users, or used to provide a specific service, during a specified period of time. These data are usually the most reliable in mature, stable programs that have a full supply of products and a robust LMIS. Strengths Forecasts based on historical consumption data usually require fewer assumptions than other types of data, in part because consumption data are already expressed in the unit of measure that is being forecasted—quantities of products dispensed to users. Usually, the fewer the assumptions, the lower the possibility for error in the forecast. Forecasts based on good quality consumption data, if available, are often the most reliable. 17 Supply chain and service delivery constraints that may have affected product availability, or access to services, are automatically reflected in historical consumption data. A supply chain cannot distribute more products for consumption than the program can procure; or that its existing warehouses, delivery systems, or staff can handle. Challenges Past consumption may not be predictive of future use, especially when new methods or products are being introduced, or when existing services or availability will be scaled up during the quantification period. In this case, the quantities based on past consumption could underestimate a forecast needed. Past consumption data may reflect periods of stock-outs, supply imbalances, or other factors that affected the availability or use of the products. Using these data could result in projections of past errors, stock-outs, or supply imbalances, rather than the quantities of products that are needed. 1.7 Projection Scenarios and Baseline input data 1.7.1 Base Population and fertility, mortality assumptions For commodity projection, we used the DemProj (DemProj 2008) model to calculate the number of women of reproductive age developed by Futures Group and the Research Triangle Institute. However, the base population of the model is taken from Population and Housing Census 2011 (Census 2011) given in Table 1.1. The life expectancy for male is 67 years and for female is 69 years [Sample Vital Registration System (SVRS 2009)] in base year (2011). Life expectancy at birth for males is assumed to be 69 years and for females is 71 years with a view to averaging longevity which will be 70 in 2021 under the national strategic plan (GoB 2012). The sex ratio at birth is assumed to be 105. TFR: 2.3 in 2011 (BDHS 2011) and 1.7 target (set in the Perspective Plan Projection) for 2021 (GoB 2012). The mortality input to DemProj, life expectancy at birth, indicates overall mortality in a population. But DemProj also needs the pattern of mortality in order to produce mortality rates by age group. Specifically, the rates required by DemProj are survival ratios, which will survive one age group into the next five year group. The best way is to use data on age specific mortality for a country with the mortality pattern at the corresponding level of life expectancy for each of the model tables. The UN South Asian model life table is considered for this exercise. 18 Table 1.1: Adjusted Population by Age and sex: Bangladesh 2011 Age group 0-4 5-9 10-14 15-19 20-24 25-29 30-34 35-39 40-44 45-49 50-54 55-59 60-64 65-69 70-74 75-79 80+ Total Male 7940842 9691237 8957038 6769650 6008978 6474284 5282247 4885149 4451977 3497551 3070186 2000104 2163739 1195016 1253976 507585 830820 74980379 Female 7717178 9200703 8350602 6606392 7822601 7543339 5636625 5052596 4139048 3136646 2702632 1639914 1925885 1001994 1065773 401647 848398 74791973 Total 15658020 18891940 17307640 13376042 13831579 14017623 10918872 9937745 8591025 6634197 5772818 3640018 4089624 2197010 2319749 909232 1679218 149772352 For commodity projection, we used the FamPlan (Spectrum) model under different scenario and assumptions. The different input data for this projection model are given below: 1.7.2 Method Mix The contraception prevalence rate among currently married women has been increased from 49 percent in 1996-97 to 61 percent in 2011 (Table 1.2). The use of modern methods is increased by 5 percentage points in the past four years from 47 percent in 2007 to 52 percent in 2011. The following table shows that the proportion of pill users increased about 10 percent during the last two decades. But in the last decade it is increased only by 4 percent. The acceptance of permanent methods such as female sterilization and male sterilization are constant over the last decade. It is also observed that the acceptance of condom and injectables has increased slightly during recent years. Similar increases were observed for Implant and Norplant as well. The decline in the acceptance of IUDs from 2.2 percent to 0.7 percent indicates that the method has been losing popularity quite rapidly among potential clients. We assumed that the method mix of 2011 will continue over the whole projection period i. e. (2014-2021). 19 Table 1.2: Change in the Contraceptive Method Mix since 1996-97 BDHS to 2011 BDHS Methods Any modern method Pill IUD Implants Injectables Condom F Sterilization M Sterilization Any traditional Periodic Abstinence Withdrawal Others Total 1996-97 BDHS 41.5 20.8 1.8 0.1 6.2 3.9 7.6 1.1 7.7 5 1.9 0.8 49.2 199-2000 BDHS 43.4 23.0 1.2 0.5 7.2 4.3 6.7 0.5 10.4 5.4 4.1 0.9 53.8 2004 BDHS 47.3 26.2 0.6 0.8 9.7 4.2 5.2 0.6 10.7 6.5 3.6 0.6 58.0 2007 BDHS 47.3 28.5 0.9 0.7 7.0 4.5 5.0 0.7 8.4 4.9 2.9 0.6 55.7 2011 BDHS 51.9 27.2 0.7 1.1 11.2 5.5 5.0 1.2 9.2 6.9 1.9 0.4 61.1 1.7.3 Contraceptive Effectiveness Table below (1.3) shows the effectiveness of different methods of contraception. The effectiveness of pills is assumed to be 92%, because both workers and clients do not know about the proper use of pills i.e. they are unaware of what to do if clients miss one or two or three pills. This increases the method failure in defining the effectiveness of pills. In the absence of any direct estimates of contraceptives effectiveness, we use the contraceptive effectiveness suggested by Bongaarts (Bongaarts and Potter l983), which appears in the accompanying Table. The effectiveness of each method will be constant over the projection period. Table 1.3 Contraceptive Effectiveness by Method Methods Condom Female sterilization Injectable IUD Male sterilization Implant Pill Traditional Other Source: Spectrum (FamPlan) Manual Effectiveness 81 100 100 96 100 100 92 50 50 1.7.4 Contraceptive Commodities Requirement per CYP For estimating couple year protection (CYP), the following attributes are used. It has been assumed that 120 pieces of condoms, 15 cycles of pills and 4 doses of injectables are required per couple years of protection (CYP). Previously, IUD retention rate was 5 years. The average age of male sterilization is assumed to be 36 and average age at female sterilization is assumed 20 to be 27 years respectively. The mean duration of use of IUD and implant are assumed 3.5 years each (Table 1.4). Table 1.4: Contraceptive Commodities Requirements per CYP Commodities Requirement per CYP Condoms/CYP 120 Female Ster. average age 27 Injections/CYP 4 IUD duration of use (yrs) 3.5 Male Ster. average age 36 Implant duration of use (yrs) 3.5 Pill cycles/CYP 15 Source: Spectrum (FamPlan) Manual 1.7.5 Percentage of Women in Union and Postpartum Insusceptibility After analyzing BDHS data it is assumed that 80% of the women are to be sexually active and this remains constant over the projection period. Among the proximate determinants of fertility, duration of breastfeeding plays an important role. The mean duration of postpartum insusceptibility has decreased slightly during 2000-2011 period. The mean duration of postpartum insusceptibility for the forecasting period is assumed 8.5 months. 1.7.6 Abortion/MR rate In developing countries like Bangladesh, it is very difficult to obtain a good empirical estimate of the proportion of unwanted pregnancies which terminate in induced abortions. This type of information needs to come from surveys—but abortions are notably underreported in surveys, especially in countries where abortion is illegal and/or is socially disapproved. Due to uncertainty regarding the estimation of abortion, we assume that the abortion rate of 0.1, estimated in 2011, would continue to remain unchanged during the projection period. 1.7.7 Sterility Co-efficient The sterility co-efficient is set 1.7% for the whole projection period (2014-2021). 1.7.8 Projection Scenarios To meet the objectives, the study sets a number of simulations for accurate estimates of the family planning commodities. Applying the projection tools with the input data, the study explore the number of user as well as required commodities in each of the following scenario. They are: Scenario-I: Unmet need for family planning will be satisfied by 2016 Scenario-II: If CPR will be 72% and traditional method shift to modern method by 2021 Scenario-III: If CPR will be 80% (Current CPR + Percent women intent to future use) by 2021 Scenario-IV: If we achieve TFR=1.7 per woman by 2021 21 1.8 Data Collection Data collected from various sources like NIPORT, DGFP, DGHS, UNFPA, Department of Statistics, University of Dhaka, Bangladesh Bureau of Statistics (BBS), Ministry of Health & Family Welfare (MOHFW), and NGOs working in the sector. It was also necessary to procure/purchase some documents and materials from market other than the collections from aforementioned sources. Browsing internet for collection and cross-checking of information/data/statistics collected/received were profusely used in order to make a full-proof projection. Consultations were held, off and on, with various stakeholders including NIPORT to extract their outlook, opinions, suggestions, recommendations and approach with regard to various indicators, methods, approach and technical points surrounding the quantification of the commodities. 1.9 Data Processing and Analysis Data collected were organized and fed into computer for systematic analysis and output generation. The system analyst worked in close connection with the study team to design the data analysis format and generate output to help the study team make desired recommendations and report. Spectrum and MS Excel were used to analyze and producing report for this study. 22 CHAPTER 02 FINDINGS 2.1 Introduction The main objective of this chapter is to create different pragmatic projection scenarios and estimate the contraceptive commodities requirements and outline the strategies to achieve demographic objectives. Contraceptive acceptors, contraceptive users and contraceptive commodity requirements are projected considering various assumptions associated with the fertility goal. 2.2 Projected number of users and acceptors according to scenario-I The objective of this chapter is to develop year-wise Family Planning Commodity Projections for 2014-2021 in Bangladesh assuming that all unmet need for family planning will be satisfied by 2016 as specified in the HPNSDP, and it should also be based on the medium variant projections of the United Nations Population Division-projections that assume a more gradual contraceptive prevalence increase that is based on historical trends. We first raised question on what would be the requirement of contraceptive commodity if unmet need for contraception (both spacers and limiters) as found in the 2011 BDHS are captured as users between 2011 and 2016. In order to meet these objectives the baseline input data and the method attributes were used. The associated summary outputs for the first goal i.e. scenario-I is shown in Table-2.l. The summary table for output shows that if unmet need for contraception can be converted into users effectively, then contraceptive acceptors will increase from about 421.7 thousand in 2014 to 721.2 thousand in 2021 and the users will increase from 22.35 million in 2014 to 29.75 million in 2021. Table 2.1: Projected number of women of reproductive age (WRA), married women of reproductive age (MWRA) and number of family planning (FP) methods user according to scenario-I in period 2014-2021 Year WRA (in Million) MWRA (in Million) User (in Million) Acceptor (in thousand) 2014 42.81 34.25 22.35 421.7 2015 43.87 35.10 23.37 437.6 2016 44.93 35.94 24.42 452.7 2017 45.97 36.77 25.48 634.9 2018 46.98 37.58 26.55 656.1 2019 47.96 38.37 27.63 676.6 2020 48.90 39.12 28.70 695.6 2021 49.79 39.83 29.75 721.2 Figure 2.1: Projected WRA, MWRA and FP methods user under scenario-I for 2014-2021 23 60 50 In Million 40 45 44 43 35 34 30 38 38 37 36 23 25 22 24 27 2014 2015 2016 2017 2018 50 49 48 47 46 39 40 28 29 30 2019 2020 2021 20 10 0 WRA MWRA User If we achieve the first simulation by 2016, the condom users will increase from 2.01 million in 2014 to 2.68 million in 2021 (Table 2.2). Table 2.2 also shows that the LAPM users will also increase from 2.95 million in 2014 to 3.94 million in 2021. Table 2.2: Projected number of family planning (FP) methods user by specific method (under assumptions scenario I) in period 2014-2021 (in Million) Method Condom Female sterilization Injectables IUD Male sterilization Implant Oral Pill Traditional Total 2014 2.01 2015 2.1 2016 2.2 2017 2.29 2018 2.39 2019 2.49 2020 2.58 2021 2.68 1.83 4.07 0.27 1.92 4.25 0.28 2 4.45 0.29 2.09 4.64 0.31 2.18 4.83 0.32 2.27 5.03 0.33 2.35 5.22 0.34 2.44 5.42 0.36 0.45 0.4 9.97 3.35 22.35 0.47 0.42 10.43 3.51 23.37 0.49 0.44 10.89 3.66 24.42 0.51 0.46 11.37 3.82 25.48 0.53 0.48 11.84 3.98 26.55 0.55 0.5 12.32 4.14 27.63 0.57 0.52 12.8 4.3 28.7 0.6 0.54 13.27 4.46 29.75 24 Figure 2.2: Projected number of methods acceptors under scenario-I for 2014-2021 800 700 635 656 677 696 2018 2019 2020 721 In thousand 600 500 422 438 453 2014 2015 2016 400 300 200 100 0 2017 2021 Year Figure 2.3 Projected Short acting method users by specific method under scenario-I for 20142021(in Million) 14 12 In million 10 10 10 12 11 11 13 13 12 8 Oral Pill 6 4 4 4 3 2 4 4 2 5 4 2 5 4 5 4 2 2 5 4 2 5 4 3 4 3 0 2015 2016 2017 2018 Year 25 2019 2020 Injectables Traditional 2 2014 Condom 2021 Figure 2.4 Projected Long-acting and permanent method users by specific method under scenario-I for 2014-2021(in Million) 3.0 2.5 In million 2.0 1.8 2.2 2.1 2.0 1.9 2.3 2.4 2.4 Female sterilization 1.5 Male sterilization IUD 1.0 0.5 0.5 0.4 0.3 0.5 0.4 0.3 0.5 0.4 0.3 0.5 0.5 0.3 0.5 0.5 0.3 0.6 0.5 0.3 0.6 0.5 0.3 2014 2015 2016 2017 2018 2019 2020 0.6 0.5 0.4 2021 Implant 0.0 Year 2.3 Projected family planning commodities requirements according to scenario-I The contraceptive commodity requirements under the assumption that if all unmet need will be satisfied by 2016 clearly demonstrate that demographic target can be achieved. Table 2.3 shows the method specific requirements. If unmet need for contraception is achieved by 2016, the estimated condom required for the year 2014 and 2021 are 241.4 million and 321.3 million respectively. The required number of oral pill for the projected period is 1393.3 million. The other commodities such as injectables, IUD and Implant required for the projected period are 151.6 million, 0.82 million and 1.22 million respectively. The required commodities by sources are shown in Appendix table-3. Table 2.3: Projected number of family planning (FP) commodities under Scenario-I in period 2014-2021 (in Million) Method Condom Injectable IUD Implant Oral Pill 2014 241.4 16.3 0.09 0.13 149.5 2015 252.5 17.0 0.09 0.14 156.4 2016 263.8 17.8 0.10 0.14 163.4 2017 275.2 18.6 0.10 0.15 170.5 26 2018 286.8 19.3 0.10 0.16 177.6 2019 298.4 20.1 0.11 0.16 184.8 2020 309.9 20.9 0.11 0.17 192.0 2021 321.3 21.7 0.12 0.17 199.1 Total 2249.2 151.6 0.82 1.22 1393.3 Figure 2.5: Projected number of FP commodities (short acting) under Scenario-I for 2014-2021 (in Million) 350 300 In million 250 252 241 200 199 192 185 178 170 163 156 150 287 275 264 321 310 298 150 100 50 16 17 18 19 19 20 21 22 0 2014 2015 2016 2017 Condom Oral Pill 2018 2019 2020 2021 Injectable 2.4 Projected number of method users and acceptors according to scenario-II [If CPR will be 72% and traditional method shift to modern method by 2021] The objective is to assess what would be the contraceptive commodity requirements if we achieve CPR=72 by 2016 and traditional method shift to modern method in 2021. The summary results of the projection are given Table 2.4. As expected, there will be no change in the women in the reproductive ages and the currently married women. The only change will occur in the contraceptive acceptors, users and the commodity requirements. Table 2.4 also shows the number of acceptors and users. The projected data imply that more acceptors and users will be required to achieve replacement fertility by 2021. For instance, new acceptors need to be increased from 480.0 thousand in 2014 to 872.5 thousand in 2021, while users need to be increased from 22 million to over 28 million during the projected period. 27 Table 2.4: Projected number of women of reproductive age (WRA), married women of reproductive age (MWRA) and number of family planning (FP) methods user according to scenario-II in period 2014-2021 WRA (in Million) MWRA (in Million) User (in Million) 42.81 43.87 44.93 45.97 46.98 47.96 48.90 49.79 34.25 35.10 35.94 36.77 37.58 38.37 39.12 39.83 22.07 23.00 23.94 24.89 25.84 26.80 27.75 28.68 Year 2014 2015 2016 2017 2018 2019 2020 2021 Acceptor (in thousand) 480.0 504.5 528.4 733.2 766.7 799.8 831.6 872.5 Figure 2.6: Projected long acting commodities under scenario-I for 2014-2021 180 160 In thousand 140 120 130 120 140 130 120 100 80 80 2014 2015 90 90 90 2016 2017 2018 140 100 150 100 160 100 80 60 40 20 0 Implant 2019 2020 2021 IUD Contraceptive commodity requirement for various methods will vary and are shown in Table 2.5. The table shows the projected users by contraceptive method mix for different methods. Results indicate an increase in users of pills, injectables, implants, and permanent methods. If the traditional method can be shifted to modern method by 2021, the total method users will increase to 22.1 million in 2014 and 28.7 million in 2021. Among them, 19.8 million and 28.7 million couples will be modern method users in 2014 and 2021 respectively. The results also indicate that the total cumulative modern method users during the projected period will be 203 million. 28 Table 2.5: Projected number of family planning (FP) method’s users by specific method (under assumptions scenario II) in period 2014-2021 (in Million) Year Condom Female sterilization Injectables IUD Male sterilization Implant Oral Pill Traditional Total 2014 2.1 2015 2.2 2016 2.3 2017 2.5 2018 2.6 2019 2.8 2020 2.9 2021 3.0 1.9 4.2 0.28 2.0 4.5 0.3 2.1 4.7 0.31 2.3 5.0 0.33 2.4 5.3 0.35 2.5 5.6 0.37 2.6 5.9 0.39 2.8 6.1 0.4 0.46 0.42 10.4 2.3 22.1 0.49 0.44 11.0 2.1 23.0 0.52 0.47 11.6 1.8 23.9 0.55 0.5 12.3 1.5 24.9 0.58 0.52 13.0 1.2 25.8 0.61 0.55 13.6 0.8 26.8 0.64 0.58 14.3 0.4 27.8 0.67 0.61 15.1 0.0 28.7 If we achieve CPR=72 and traditional method shifted to modern method, it clearly demonstrates that demographic target i.e replacement fertility can be achieved. The results are shown in Appendix Table 2. 2.5 Projected family planning commodities requirements according to scenario-II Contraceptive commodity requirement for various methods will vary and are shown in Table 2.6. By applying CYP of each method, the required condom, injectables, IUD, implant and oral pill for the projected period are 2451.4 million, 165.2 million, 0.93 million, 1.38 million and 1518.5 million respectively (Table 2.6). Table 2.6: Projected number of family planning (FP) commodities under Scenario-II in period 2014-2021 (in Million) Method Condom Injectable s IUD Implant Oral Pill 2014 251.0 2015 265.9 2016 281.4 2017 297.3 2018 313.7 2019 330.4 2020 347.3 2021 364.4 Total 2451.4 16.9 0.1 0.14 155.5 17.9 0.1 0.15 164.7 19.0 0.11 0.16 174.3 20.0 0.11 0.17 184.2 21.1 0.12 0.18 194.3 22.3 0.12 0.19 204.7 23.4 0.13 0.19 215.2 24.6 0.14 0.2 225.7 165.2 0.93 1.38 1518.5 If all unmet need will be converted into users by 2016, it clearly demonstrates that demographic target i.e. replacement fertility can be achieved. We also estimated contraceptive requirement by sources if unmet need for contraception is achieved by 2016. The results are shown in Appendix Table 5. 29 Figure 2.7: Projected number of short acting family planning (FP) commodities under Scenario-II 400 350 In million 300 261 247 250 200 214 205 196 187 179 170 162 153 303 288 274 345 331 317 150 100 50 17 18 19 19 20 21 22 23 2014 2015 2016 2017 2018 2019 2020 2021 0 Condom Injectables Oral Pill Figure 2.8: Projected number of family planning (FP) Long-acting commodities under Scenario-II 200 180 In thousand 160 140 150 170 160 150 140 120 100 90 100 100 110 110 170 120 180 120 190 130 80 60 40 20 0 2014 2015 2016 2017 IUD 2018 Implant 30 2019 2020 2021 2.6 Projected number of method users and acceptors according to scenario-III [If CPR will be 80% (Current CPR + Percent women intent to future use) by 2021] The BDHS data show that 61.2% of the currently married were the current users and 38.8% never users. The never users were asked whether they intend to use in future. Among the nonusers about 65% reported that they intend to use in future. In our projection, among these 65% intenders of future use being converted into users by 2021, the total users will stand for approximately 80%. If this can be implemented, then the associated acceptors, users and commodity requirements will stand as shown in Table 2.7 and Table 2.9. If we achieve this demographic goal, new acceptors need to be increased from 456.5 thousand in 2014 to 801 thousand in 2021 while users need to be increased from 22.9 million to over 31 million during the projected period. Table 2.7: Projected number of women of reproductive age (WRA), married women of reproductive age (MWRA) and number of family planning (FP) methods user according to scenario-III in period 2014-2021 Year WRA (in Million) MWRA (in Million) User (in Million) 2014 2015 2016 2017 2018 2019 2020 2021 42.81 43.87 44.93 45.97 46.98 47.96 48.90 49.79 34.25 35.10 35.94 36.77 37.58 38.37 39.12 39.83 22.89 24.12 25.38 26.65 27.95 29.25 30.56 31.86 Acceptor (in thousand) 456.5 476.5 495.6 689.9 716.9 743.1 768.0 801.0 The table 2.8 shows the projected users by contraceptive method mix for different methods. Results indicate an increase in users of pills, injectables, implants, and permanent methods. If the future intender can be shifted to modern method by 2021, the total method users will increase to 22.9 million in 2014 and 31.9 million in 2021. Among them, 3.02 million and 4.22 million couples will be LAPM users in 2014 and 2021 respectively. 31 Table 2.8: Projected number of family planning (FP) methods user by specific method (under assumptions scenario III) in period 2014-2021 (in Million) Method Condom Female sterilization Injectables IUD Male sterilization Implant Oral Pill Traditional Total 2014 2.06 2015 2.17 2016 2.29 2017 2.4 2018 2.52 2019 2.64 2020 2.76 2021 2.88 1.88 4.17 0.27 1.98 4.39 0.29 2.08 4.63 0.3 2.19 4.86 0.32 2.3 5.1 0.34 2.41 5.34 0.35 2.51 5.58 0.37 2.62 5.82 0.38 0.46 0.41 10.22 3.42 22.89 0.48 0.43 10.77 3.59 24.12 0.51 0.46 11.33 3.77 25.38 0.53 0.48 11.91 3.96 26.65 0.56 0.5 12.49 4.14 27.95 0.59 0.53 13.08 4.32 29.25 0.61 0.55 13.67 4.51 30.56 0.64 0.58 14.26 4.69 31.86 2.7 Projected family planning commodities requirements according to scenario-III Contraceptive commodity requirement for various methods will vary and are shown in Table 2.9. By applying CYP of each method, the required condom, injectables, IUD, implant and oral pill for the projected period are 2366.7 million, 159.5 million, 0.9 million, 1.35 million and 1466.1 million respectively (Table 2.9). Table 2.9: Projected number of family planning (FP) commodities under Scenario-III in period 2014-2021 (in Million) Method 2014 Condom Injectable s IUD Implant 247.42 Oral Pill 153.26 16.68 0.09 0.14 2015 260.7 8 17.58 0.1 0.15 161.5 4 2016 2017 2018 2019 2020 2021 Total 274.47 288.4 302.52 316.76 331.07 345.31 2366.7 18.5 0.1 0.15 19.44 0.11 0.16 20.39 0.11 0.17 21.35 0.12 0.17 22.32 0.12 0.18 23.28 0.13 0.19 159.5 0.9 1.3 170.02 178.65 187.39 196.22 205.08 213.9 1466.1 Compared to other two goals, both users and acceptors will be slightly higher from the scenario I, if intenders could be converted into users. This is attributed to the fact that the rate of use to be increased. This is also reflected in the present projection. The associated demographic impact is also expected to be improved. For instance, the associated contraceptive prevalence rate will be 80% in 2021 and implied TFR will be 1.3. The result is given in Appendix Table 7. 32 Figure 2.9: Projected number of short term family planning (FP) commodities under Scenario-III 400 350 In million 300 250 261 247 200 214 205 196 187 179 170 162 153 303 288 274 345 331 317 150 100 50 17 18 19 19 20 21 22 23 2014 2015 2016 2017 2018 2019 2020 2021 0 Condom Injectables Oral Pill Figure 2.10: Projected number of long-acting family planning (FP) commodities under Scenario-III 400 350 In million 300 250 274 261 247 200 214 205 196 187 179 170 162 153 317 303 288 345 331 150 100 50 17 18 19 19 20 21 22 23 2014 2015 2016 2017 2018 2019 2020 2021 0 Condom Injectables 33 Oral Pill 2.8 Projected number of method users and acceptors according to scenario-IV [If TFR=1.7 will achieve by 2021] Table 2.10 shows that the projected number of women of reproductive age, married women of reproductive and family planning method user will be 42.8 million, 34 million and 22 million respectively in 2014 under the assumption that current TFR will be 1.7 by 2021. Table 2.10 also shows that projected users will be 28.9 million and acceptor will be 691 thousand by 2021. Table 2.10: Projected number of women of reproductive age (WRA), married women of reproductive age (MWRA) and number of family planning (FP) methods user in period 2014-2021 (in Million) Year 2014 2015 2016 2017 2018 2019 2020 2021 WRA 42.81 43.87 44.93 45.97 46.98 47.96 48.90 49.79 CMWRA 34.25 35.10 35.94 36.77 37.58 38.37 39.12 39.83 FP User 22.14 23.09 24.05 25.02 26.00 26.98 27.95 28.91 Acceptor 408.4 422.8 436.3 614.0 633.0 651.3 668.2 691.1 The projected number of user by contraceptive method mix for different methods given in Table 2.11 indicates an increase in users of pills, injectables, implants, and permanent methods. If the method mix of 2011 continues through 2014-2021, the total method users will be increased to 22.14 million in 2014 and 28.9 million in 2021. Among them, 18.8 million and 24.6 million WRA will be modern method users in 2014 and 2021 respectively. Table 2.11: Projected number of specific family planning (FP) methods user (under Scenario-IV) in period 2014-2021 (in Million) Method 2014 2015 2016 2017 2018 2019 2020 2021 Condom 1.99 2.08 2.16 2.25 2.34 2.43 2.52 2.6 Female sterilization 1.82 1.89 1.97 2.05 2.13 2.21 2.29 2.37 Injectables 4.03 4.2 4.38 4.55 4.73 4.91 5.09 5.26 IUD 0.27 0.28 0.29 0.3 0.31 0.32 0.34 0.35 Male sterilization 0.44 0.46 0.48 0.5 0.52 0.54 0.56 0.58 Implant 0.4 0.42 0.43 0.45 0.47 0.49 0.5 0.52 Oral Pill 9.87 10.3 10.73 11.16 11.6 12.03 12.47 12.9 Traditional 3.32 3.46 3.61 3.75 3.9 4.05 4.19 4.34 Total 22.14 23.09 24.05 25.02 26 26.98 27.95 28.91 2.9 Projected family planning commodities requirements according to scenario-IV Based on CYP attributes, we estimated that 2205 million condoms, 1366 million cycles of pills, and 148.6 million doses of injectables are required for 2014-2021. The other commodities are 34 implants (one and two-rod) and IUDs at 1.16 million and 80 thousand, respectively, for 20142021 (Table 2.12). Table 2.12: Projected number FP Commodities (under scenario-IV) in period 2014-2021 (in Million) 2014 2015 2016 2017 2018 2019 2020 2021 Total Condom 239.11 249.33 259.75 270.26 280.82 291.39 301.91 312.26 2204.8 Injectables 16.12 16.81 17.51 18.22 18.93 19.64 20.35 21.05 148.6 IUD 0.09 0.09 0.09 0.1 0.1 0.1 0.11 0.11 0.80 Implant 0.13 0.14 0.14 0.15 0.15 0.16 0.16 0.17 1.2 Oral Pill 148.11 154.45 160.9 167.41 173.95 180.5 187.02 193.43 1365.8 The required commodities by sources are given in appendix (Table-9) 35 CHAPTER 03 CONCLUSION AND POLICY IMPLICATIONS Introduction The immediate vision of Bangladesh Family Planning Program is to achieve replacement level of fertility. If it can be achieved, what would be contraceptive commodity requirements? To assess this, several scenarios were drawn up and contraceptive requirements are projected for 2014 to 2021. The baseline and input data including proximate determinants are discussed in terms of their contributions in fertility reductions. Because of variation in the theme of the assumptions, the users, acceptors and contraceptive commodity requirements also varied. The important question is which strategy or strategies should be used to achieve demographic objectives of the government and the associated contraceptive requirements need to be debated on, on the basis of past experiences. 3.2 Reducing Unmet Need for Contraception for Limiters and Spacers Converting unmet need for limiters and spacers into users have significant impact on the achievement of demographic goal because of the fact that if they can be converted into users, the contraceptive use rate will be about 74.7%. If this can be achieved, Bangladesh will be able to achieve replacement fertility immediately. If we put this CPR in the regression line TFR = 7.15 - 0.0688 CPR, then TFR will be 2.0 children per woman (which is the replacement fertility) and corresponding population growth will be zero percent (zero population growth). The contraceptive requirement will vary by methods, with pill and condom dominating in it. The quality strategy, without emphasizing specific targets, will help increase contraceptive prevalence rate from the current 61 to 74.7 by 2021 if unmet need for contraception can be reduced, and, consequently, it will lower the fertility rate from 2.0, suggesting that replacement fertility will be achieved. 3.3 Transforming Intenders into Users Converting intenders have more demographic impact than reducing unmet need for contraception. The reason for this is that the majority of the intenders will be modern temporary method users and some of them may be traditional method users. The total CPR will be 80% and corresponding TFR will be less than 2.00. However, to convert intenders into users, the important strategic issues to be given top priorities are: identification of intenders (among the never-users who intended to use in future and converting them into users) and client segmentation, special IEC, procurement of additional contraceptives and supplies, more efficient management of services (e.g., management of side-effects). Identification of intenders should be based on an understanding of the general and spatial characteristics of the intenders. Segmentation analyses of the intenders who intend to use fertility intention are the two best predictors. Intensive field-worker visits to intenders can accelerate the process of transforming intenders into effective users. 3.4 Shifting Traditional Method toward Modern Methods The scenario II increased use of modern methods--has demonstrative effect on the achievement of replacement fertility. This is due to the fact that CYP for modern method user is much higher than traditional methods including injectable methods. Increased use of LAPM also 36 means that contraceptive requirements for pill and condom will be lower and, therefore, will reduce cost of burden. The trend analysis of BDHS data indicates that long-acting method use in family planning program has been declining, partly because of side-effect and partly because that it does not allow for privacy, and suffers from shortage of supplies, equipment and physicians. If the programs fail to motivate users to LAPM, contraceptive requirements, under this scenario, will be much higher and it will not be cost-effective. 3.5 Achieve TFR= 1.7 per woman Bangladesh has achieved a considerable decline in fertility from high 6.3 births per woman in the 1970s to 2.3 births per woman in 2011. Several researchers argued that this fertility decline in Bangladesh was achieved primarily owing to a successful family planning program. There are substantial variations in the level of fertility among the six Divisions. Khulna (South-West) Division achieved replacement level fertility in 2011. But differential is larger across Divisions, with the Eastern part (Chittagong and Sylhet Divisions) representing higher fertility than the Western part (Khulna and Rajshahi Divisions) of the country. The women in Sylhet Division had on the average 1.2 more children than women in Khulna Division, and also the women in Chittagong Division had 1.0 more children than that of Khulna Division. Khulna and Rajshahi Divisions have achieved replacement level of fertility and high levels of contraceptive prevalence rates. This suggests that if replacement fertility in Chittagong Division and Sylhet Division is achieved, then country will have fertility below replacement levels. The spectrum policy model indicates that if TFR=1.7 is achieved by 2021, CPR will attain 73%. This will also fulfil the demographic goal (below replacement fertility) and targeted CPR for the country as a whole. 3.6 Formulating the Quality Strategy Given the vision for the Bangladesh family planning program over the next 8 years, quality strategy could be an important determinant for the fulfillment of the family planning and population goals. There are two major components of the quality strategy. The first focuses on making family planning services accessible to current non-users who intend to use in future. This means that regular visit of field workers should be ensured. One concern is that over the last few years (BDHSs) visit of field workers at the household level has been declining despite the fact that contraceptive prevalence rate has been increasing. The second component emphasizes substantially improving the quality of family planning services for all users. The quality strategy stipulates that the family planning program should find ways to reach these women intenders (or women who have unplanned pregnancies, mistimed births and unwanted pregnancies) and help them to get their expressed desires fulfilled. The Information, Education and Communication (IEC) program in place may need to be reviewed, redesigned and made multi-faceted to have effective and measureable impact on the point of reaching the non-users. The program strategy should be to reduce the incidences of the above mentioned events and it would help to achieve demographic objectives. In addition to converting the intenders into users, this strategy requires gradual improvement in contraceptive continuation and effectiveness as well as gradual shift in method mix toward longterm method acceptance, and method mix. This information suggests that encouraging for LAPM use will not only have demonstrative effect on the achievement of replacement level fertility, but also will lower requirement of contraceptive commodities. New strategy is required to be so designed as to help increase LAMP acceptors, because current use of LAPM is significantly low. 37 3.7 Policy Implications The commodity projection is performed for four scenarios. The findings indicate that first scenario provides projected contraceptive commodities that are very close to actual figures from MIS data. This also fulfills the expected demographic goal. If programmatic inputs are provided to increase the number of acceptors of LAPM users, then projected requirement need to be modified based on MIS and service statistics data. However, current situation does not indicate that any major deviation from projected requirements is likely to take place during next few years. The family planning commodity projection will be successful if FP program implements according to strategic plan, timely procure and supply. To minimize any risk of a future stockout, the projected requirements for contraceptive commodities need to adjust for current consumption data. In addition, the projected number of condoms needs to adjust for increased demand for condoms for future STD, HIV/AIDS prevention program. The FP commodity projection presented in this paper provides guideline for policymakers to understand the probable scenario likely to prevail during the projected period. However, the expected scenario can be changed through additional program input or change in population characteristic. The future commodity requirement can also change/modify based on input data from future survey. 3.8 Limitations Due to lack of information on ECP, the projection for this commodity is not done There are rules for distributing DDS kits at the clinics level. Therefore, projection for DDS kits remains a challenge. Projected number of condoms may not meet the demand because it depends on future STD, HIV/AIDS prevention program. 3.9 Recommendation To reduce the cumulative pressure of contraceptive commodity of short-acting methods the country need to shift contraceptive use patterns towards more effective longer-acting and permanent methods. Multi-sectoral efforts for raising female age at marriage and delaying age at first birth through promoting female education (including female school/college stipend program) and creating employment opportunities, and more effective enforcement of the legal age of marriage could help achieve the demographic goal. Intensifying public information and motivation campaigns to bring about overall changes in attitude and awareness creation among all stakeholders on: longer acting and permanent methods, delayed marriage, popularizing two-child family norm, minimizing drop-out and unwanted pregnancy, male involvement in NSV, availability of FP services, female education etc will produce definable results on a longer term. Finally, if we want to achieve replacement fertility by 2016 and population stabilization, several factors should be taken into consideration. These include: High population momentum effects; Low age at marriage; High adolescent fertility; Shifting of child bearing towards younger ages; Decline in birth interval from marriage to first birth interval; 38 Continuous decline in permanent methods and long acting methods such as sterilization and IUD; and Decline in the visit of households by family planning workers. To deal with all the above-mentioned factors an all-out multi-sectoral approach would be required to reduce the population momentum and to reach population stabilization even we achieve demographic goal by 2016. 39 BIBLIOGRAPHY Bangladesh Bureau of Statistics. 2012. Bangladesh Population Census, 2011. Preliminary Report. Dhaka: Bangladesh Bureau of Statistics, Planning Division, Ministry of Planning. www.bbs.gov.bd Bangladesh Bureau of Statistics. 2010. Sample Vital Registration System; Planning Division, Ministry of Planning. Bongaarts, J. and G. R. Potter. 1983. Fertility, Biology, and Behavior: An Analysis of the Proximate Determinants. Academic Press, New York. Government of Bangladesh. 1998. Statistical Yearbook of Bangladesh 1997, Dhaka: Bangladesh Bureau of Statistics. Government of Bangladesh. 2012. Prospective Plan of Bangladesh 2010-2021, Dhaka: General Economic Division, Planning commission. DGFP Monthly Logistics and Family Planning, Maternal and Child Health and RH Services Reports, 2011, MIS unit, Dhaka: DGFP, Ministry of Health and Family Welfare. www.dgfp.gov.bd DemProj. Spectrum System of Policy Models. 2008. A Computer Program for Making Population Projections. USAID | Health Policy Initiative. FamPlan. Spectrum System of Policy Models. 2008. A Computer Program for Projecting Family Planning Requirements. USAID | Health Policy Initiative. Ministry of Health and Family Welfare (Bangladesh). 2011. Strategic Plan for Bangladesh National Family Planning Programme 2012-2016. www.mohfw.gov.bd BDHS 1996. NIPORT, Mitra and Associates, and ORC Macro. 1996-1997. Bangladesh Demographic and Health Survey,1996-1997. Dhaka, Bangladesh, and Calverton, Maryland, USA. BDHS 1999. NIPORT, Mitra and Associates, and ORC Macro. 1999-2000. Bangladesh Demographic and Health Survey,1999-2000. Dhaka, Bangladesh, and Calverton, Maryland, USA. BDHS 2004. NIPORT, Mitra and Associates, and ORC Macro. 2005. Bangladesh Demographic and Health Survey 2004. Dhaka, Bangladesh, and Calverton, Maryland, USA. BDHS 2007. NIPORT, Mitra and Associates, and Macro International. 2009. Bangladesh Demographic and Health Survey 2007. Dhaka, Bangladesh, and Calverton, Maryland, USA. BDHS 2011. NIPORT, Mitra and Associates, and ICF international. 2011. Bangladesh Demographic and Health Survey 2011 Preliminary Report. Dhaka, Bangladesh, and Calverton, Maryland, USA. Mridha, M. K., I. Anwar, and M. Koblinsky. 2009. Public-Sector Maternal Health Programmes and Services for Rural Bangladesh. Journal of Health and Population Nutrition. Apr. 27(2); 124-138. 40 USAID | DELIVER PROJECT, Task Order 1. 2011. The Logistics Handbook: A Practical Guide for the Supply Chain Management of Health Commodities. Arlington, Va.: USAID | DELIVER PROJECT, Task Order 1. 41 APPENDIX-A Table 1: Projected Demographic goals under scenario-I Demographic Characteristics TFR (Per woman) CPR (Percent) All method Condom Female sterilization Injectables IUD Male sterilization Implant Oral Pill Traditional 2014 2015 2016 2017 2018 2019 2020 2021 2.09 2.02 1.95 1.87 1.8 1.73 1.66 1.59 65.25 5.87 66.6 5.99 67.95 6.12 69.3 6.24 70.65 6.36 72 6.48 73.35 6.6 74.7 6.72 5.35 11.88 0.78 1.3 1.17 29.1 9.79 5.46 12.12 0.8 1.33 1.2 29.7 9.99 5.57 12.37 0.82 1.36 1.22 30.31 10.19 5.68 12.61 0.83 1.39 1.25 30.91 10.39 5.79 12.86 0.85 1.41 1.27 31.51 10.6 5.9 13.1 0.86 1.44 1.3 32.11 10.8 6.01 13.35 0.88 1.47 1.32 32.71 11 6.13 13.6 0.9 1.49 1.34 33.32 11.21 Table 2: Source Mix by method in percent Source Mix 2014 2015 Condom Public 30 30 Private 70 70 Female sterilization Public 80 80 Private 20 20 Injectable Public 75 75 Private 25 25 IUD Public 96 96 Private 4 4 Male sterilization Public 96 96 Private 4 4 Implant Public 99 99 Private 1 1 Pill Public 60 60 2016 2017 2018 2019 30 70 30 70 30 70 30 70 30 70 30 70 80 20 80 20 80 20 80 20 80 20 80 20 75 25 75 25 75 25 75 25 75 25 75 25 96 4 96 4 96 4 96 4 96 4 96 4 96 4 96 4 96 4 96 4 96 4 96 4 99 1 99 1 99 1 99 1 99 1 99 1 60 60 60 60 60 60 42 2020 2021 Private 40 40 40 40 40 40 40 40 Source: BDHS 2011 Table 3: Projected commodities by source under scenario-I Commodity 2014 2015 2016 2017 2018 2019 2020 Condom Public 72405704 75733920 79131992 82569672 86032808 89508016 92976136 Private 168946640 176712480 184641296 192662560 200743216 208852032 216944320 Injectable Public 12201702 12762570 13335206 13914519 14498122 15083758 15668202 Private 4067234 4254190 4445069 4638173 4832708 5027920 5222734 IUD Public 85418 89048 92641 96225 99786 103292 106666 Private 3559 3710 3860 4009 4158 4304 4444 Implant Public 132132 137746 143304 148847 154357 159779 164999 Private 1335 1391 1448 1504 1559 1614 1667 Pill Public 89702608 93825912 98035736 102294648 106585096 110890488 115187104 Private 59801740 62550612 65357152 68196432 71056728 73926992 76791408 Table 4: Projected Demographic goals under scenario-II Demographic Characteristics TFR (Per woman) CPR (percent) All method Condom Female sterilization Injectables IUD Male sterilization Implant Oral Pill Traditional 2014 2015 2016 2017 2018 2019 2020 2021 2.13 2.07 2.01 1.95 1.89 1.84 1.78 1.72 64.4 6.11 65.5 6.31 66.6 6.52 67.6 6.74 68.7 6.96 69.8 7.18 70.9 7.4 72 7.62 5.56 12.35 0.81 1.36 1.22 30.26 6.77 5.75 12.77 0.84 1.4 1.26 31.29 5.89 5.94 13.19 0.87 1.45 1.3 32.33 4.98 6.14 13.63 0.9 1.5 1.35 33.39 4.04 6.34 14.06 0.93 1.55 1.39 34.47 3.07 6.54 14.51 0.96 1.59 1.44 35.56 2.07 6.74 14.96 0.99 1.64 1.48 36.66 1.05 6.95 15.42 1.02 1.69 1.52 37.78 0 Table 5: Projected commodities by source under scenario-II Commodities 2014 2015 2016 2017 2018 2019 202 Condom Public 75290128 79770720 84418880 89202952 94106560 99112736 10419700 Private 175676976 186131664 196977392 208140224 219581968 231263040 24312635 Injectable Public 12687788 13442834 14226141 15032350 15858694 16702340 1755911 Private 4229263 4480945 4742047 5010784 5286232 5567447 585304 IUD Public 92445 97596 102801 108087 113437 118797 12408 Private 3852 4066 4283 4504 4727 4950 517 Implant Public 143002 150970 159020 167197 175468 183767 19194 43 Pill Private Public Private 1444 93276192 62184132 1525 1606 1689 1772 1856 193 98827008 104585608 110512584 116587576 122789712 12908849 65884664 69723736 73675056 77725048 81859816 8605900 Table 6: Projected demographic goals under scenario-III Demographic Characteristics TFR (Per Woman) CPR (Percent) All method Condom Female sterilization Injectables IUD Male sterilization Implant Oral Pill Traditional 2014 2015 2016 2017 2018 2019 2020 2021 2.0 1.9 1.8 1.7 1.6 1.5 1.4 1.3 66.84 6.02 68.72 6.19 70.6 6.36 72.48 6.54 74.36 6.71 76.24 6.88 78.12 7.05 80.0 7.22 5.49 12.17 0.8 1.34 1.2 29.83 9.98 5.64 12.52 0.83 1.38 1.24 30.68 10.24 5.8 12.87 0.85 1.41 1.27 31.53 10.5 5.95 13.22 0.87 1.45 1.31 32.39 10.76 6.11 13.56 0.89 1.49 1.34 33.24 11.01 6.27 13.91 0.92 1.53 1.38 34.09 11.27 6.43 14.26 0.94 1.57 1.41 34.95 11.52 6.58 14.61 0.96 1.61 1.44 35.8 11.77 Table 7: Projected commodities by source under scenario-III ommodities 2014 2015 2016 2017 2018 2019 2020 2021 ondom Public 74225696 78232728 82341592 86520768 90754864 95028536 99320400 1035919 Private 173193280 182543024 192130384 201881776 211761328 221733248 231747600 2417145 ectable Public 12508410 13183650 13876084 14580363 15293874 16014062 16737334 174571 Private 4169470 4394550 4625362 4860121 5097958 5338021 5579112 58190 D Public 89681 94115 98539 102980 107423 111832 116117 1211 Private 3737 3921 4106 4291 4476 4660 4838 50 mplant Public 138725 145583 152432 159297 166172 172986 179620 1873 Private 1401 1471 1540 1609 1679 1747 1814 18 l Public 91957424 96921600 102012112 107189688 112435144 117729752 123046976 1283387 Private 61304952 64614404 68008072 71459792 74956760 78486496 82031328 855591 Table 8: Projected demographic goals under scenario-IV Demographic Characteristics TFR (Per woman) CPR (Percent) All method 2014 2015 2016 2017 2018 2019 2020 2021 2.12 2.06 2 1.94 1.88 1.82 1.76 1.7 64.64 65.78 66.91 68.05 69.18 70.32 71.45 72.59 44 Condom Female sterilization Injectables IUD Male sterilization Implant Oral Pill Traditional 5.82 5.92 6.02 6.12 6.23 6.33 6.43 6.53 5.3 11.77 0.78 5.39 11.97 0.79 5.49 12.18 0.8 5.58 12.38 0.82 5.67 12.59 0.83 5.77 12.8 0.84 5.86 13 0.86 5.95 13.21 0.87 1.29 1.16 28.83 9.7 1.32 1.18 29.34 9.87 1.34 1.2 29.84 10.04 1.36 1.22 30.35 10.21 1.38 1.25 30.86 10.38 1.41 1.27 31.36 10.55 1.43 1.29 31.87 10.72 1.45 1.31 32.37 10.89 Table 9: Projected commodities by source under scenario-IV Commodities 2014 2015 2016 2017 2018 2019 202 Condom Public 71732792 74799720 77924808 81078440 84247056 87417912 90572864 Private 167376512 174532672 181824560 189183024 196576464 203975152 21133668 Injectable Public 12088304 12605139 13131774 13663220 14197190 14731539 15263206 Private 4029435 4201713 4377258 4554407 4732397 4910513 5087736 IUD Public 83806 87128 90404 93662 96889 100054 103085 Private 3492 3630 3767 3903 4037 4169 4295 Implant Public 129637 134776 139845 144883 149875 154771 159459 Private 1309 1361 1413 1463 1514 1563 1611 Pill Public 88868952 92668536 96540176 100447184 104372728 108301088 11220972 Private 59245968 61779024 64360124 66964784 69581824 72200720 74806488 45 Appendix-B Figure 1: Projected Total Population 2011-2021 170 165 161 165 168 160 160 In Million 163 166 158 156 154 155 150 152 150 145 140 2011 2012 2013 2014 2015 2016 2017 2018 2019 2020 Figure 2: Projected number method users under Scenario I 46 2021 Figure 3: Projected TFR under Scenario I Figure 4: Projected number condom under Scenario I 47 Figure 5: Projected number Injectables under Scenario I Figure 6: Projected number IUD under Scenario I 48 Figure 7: Projected number oral Pills under Scenario I Figure 8: Projected number of WRA under Scenario I Method: Prevalence (Condom) 49 Method: Prevalence (Pill) 50 51 Research Team Khandaker Rashedul Haque, PhD Team Leader Prof Nurul Islam, PhD Sociologist Prof Lutfun Nahar, PhD Demographer Dr. Abdus Sabur Health Specialist Mohammad Nurul Alam, PhD Statistician & Projection Specialist Prof. M Sheikh Giash Uddin, PhD Statistician & Projection Specialist Md Shamsul Alam Statistician & Projection Specialist Md Khan Jahan Ali Statistician & Projection Specialist Iftekhar Uddin Ahmad Team Coordination 52