doc Form
advertisement

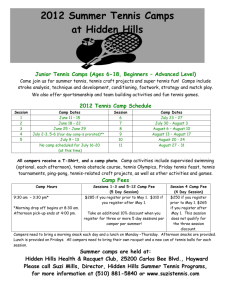
Camp Duffield Registration Form (Please print)-page A Date: _______________ Name of Camper: Last____________________________First_______________________________ Home Address:______________________________________________________________________ Street City State Zip Home Phone# ________________________Sex _______ DOB: ___/___/____ Grade Completed _____ Parents/Guardians:____________________________________________________________________ Custodial Parent Names Cell Phone# Mom:_______________________________ Dad:_________________________________ Parents email: ________________________________Camper email:___________________________ Emergency Contact Information: (If unable to reach a parent, someone who is available 24/7) Contact name___________________________Phone:___________________Relationship___________ Contact name___________________________Phone:___________________Relationship___________ Campers Physician:_________________________________ Phone_____________________________ Physicians Address: ___________________________________________________________________ Street City State Zip Circle the Camp Attending: Date of Camp Camp Paid in Full by Paid in Full by May 1st June 1st Chipmunks Parent July 12-15 Chipmunks July 12-15 $175 $200 Music July 12-18 $290 $310 Science July 12-18 $290 $310 Night Owls July 19-25 $300 $320 Office Use Only (Date Received) __________________________________________________________________________ Signature of parent or guardian Date This form must be turned in by June 1st . Duffield Summer Camps, 280 Warren Ave, Kenmore, NY, 14217 Rev.150116 Camp Duffield Registration Form (Please print)-page B Date:___________ Name of Camper: ______________________________________________DOB_____/____/______ Has camper traveled outside the country in the past 9 months? _________________________ When/Where ______________________________________________________________________ 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. 20. 21. 22. 23. 24. 25. 26. 27. Has camper had a recent injury, illness or infectious disease? Are there any chronic or recurring illness/condition? Has camper been hospitalized or had any surgery? Does camper have frequent headaches Ever had a head injury or been knocked unconscious? Wear glasses or contacts Ever had frequent ear infections? Ever pass out or been dizzy during or after exercise? Ever had seizures or convulsions? Ever had chest pains? Ever had high blood pressure? Ever been diagnosed with a heart murmur or heart condition? Ever had back problems? Ever had joint problems? Bringing an orthopedic device to camp? Have any skin problems? Have diabetes? Have asthma? Had mononucleosis in past 12 months? Had problems with diarrhea/constipation? Problems with sleepwalking or bed wetting? If female – abnormal menstrual history? Ever had a emotional problems for which professional help sought? Ever had an eating disorder? Bee sting reactions? Hay fever or other allergies? Any other facts we need to know: Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes No No No No No No No No No No No No No No No No No No No No No No No No No No No Explain yes answers here: _________________________________________ _________________________________________________________________ _________________________________________________________________ _________________________________________________________________ Authorizations: This health history is correct and complete to the best of my knowledge, and the person herein described has permission to engage in all camp activities except as noted on this form. I hereby give permission to the medical personnel selected by the Camp Director to secure proper treatment and transportation, for myself or my child named above if deemed necessary. I also give permission to share their medical information for this purpose. (This must be signed for camper to attend camp) ____________ Signature of parent or guardian Date This form must be turned in by June 1st . Duffield Summer Camps, 280 Warren Ave, Kenmore, NY, 14217 Rev.150116 Camp Duffield Registration Form (Please print)-page C Authorization from Parent/Guardian for person to Consent for treatment of minor patient I, ________________________________do hereby authorize Camp Duffield Staff to sign for any Medical Treatment deemed necessary for (print child name) ____________________________, whose birth date is __/__/_____. This authorization is valid from (date) _________ through and including _____________. Today’s Date_________________________________________ Parent/Guardian______________________________________________________ Print Parent/Guardian______________________________________________________ Signature The person herein described has appeared before me and is known by me or has presented sufficient identification to prove, that he or she, is indeed, the above individual. Notary Public Signature/Stamp/Date: _________________________________________________________________________________ Health Insurance Company____________________________________________________________ Name of insured _________________________________ Relationship to camper ________________ Identification Number _________________________________Group No._______________________ Place of Employment_________________________________________________________________ A photocopy of insurance card is required to attend camp. Camper Physician: Phone__________________________ Camper Dentist/Orthodontist: Phone__________________________ This form must be turned in by June 1st . Duffield Summer Camps, 280 Warren Ave, Kenmore, NY, 14217 Rev.150116 Physician’s Report page 1 Camp Duffield Health History Name of Camper: ____________________________________________DOB_____/_____/_____ Date of physical: _____/_____/______ (physical must be within past calendar year) Has camper been hospitalized within the past 3 years? ________________________________ If yes explain details and dates: _____________________________________________________ Patient’s: HT ________ WT ________ P ________ BP _______/_______RR ________ PHYSICAL EXAMINATION SYSTEM HEAD, NECK EARS,NOSE,THROAT LUNGS HEART ABDOMEN GENITALIA SPINE EXTREMITIES NEURO SKIN EYES WITHIN NORMAL ABNORMAL REASON MEDICATIONS Please list all medications (including over the counter or non prescription drugs) being taken. Bring enough medication to last the entire time at camp. Keep in original packaging/bottle that identifies the medication, the prescribing doctor, the dosage and frequency of administration. MEDICATION DOSAGE TIMES GIVEN Signature of Physician REASON SPECIAL INSTRUCTIONS Date_________________ Print Name or stamp _____________________________________________________________ Physician’s Report page 2 This form must be turned in by June 1st . Duffield Summer Camps, 280 Warren Ave, Kenmore, NY, 14217 Rev.150116 Camp Duffield Health History Name of Camper: ___________________________________________DOB_____/_____/_____ Date of physical: _____/_____/______ (physical must be within past calendar year) Immunization History: Provide the month and year for each immunization. All immunizations must be current. Copies of immunization forms from health-care providers are acceptable; please attach to this form. Immunization ( List or attach doctors records of immunizations ) DTaP or TdaP_________________________________________________________________ DT or TdaP___________________________________________________________________ MMR________________________________________________________________________ IVP_________________________________________________________________________ HIB_________________________________________________________________________ PCV_________________________________________________________________________ Hepatitis A___________________________________________________________________ Hepatitis B___________________________________________________________________ Varicella_____________________________________________________________________ Meningococcal________________________________________________________________ Influenza____________________________________________________________________ Pertussis_____________________________________________________________________ Allergy Information: Allergy to: Dust/Mold Insect Bites: Animals: Latex Sunscreen Food: Food: Medications: Medication: ___Does not apply (no allergies) Reaction: Treatment: If child is required to carry an epi pen, you must bring the epi pen with your physicians Rx and contact Mary Owens as we need additional forms filled out. Signature of Physician Date_________________ Print Name or stamp _____________________________________________________________ This form must be turned in by June 1st . Duffield Summer Camps, 280 Warren Ave, Kenmore, NY, 14217 Rev.150116 Physician’s Report page 3 Camp Duffield Health History Name of Camper: ___________________________________________DOB_____/_____/_____ OVER THE COUNTER MEDICATION FORM Your medical doctor must complete this form I hereby authorize that the following medications may be given to the above named camper at Camp Duffield after nursing assessment. Bactine (topical) for minor wound care, first aid as needed Triple Antibiotic Ointment (topical) for wound healing Tylenol (oral) as directed on bottle Ibuprophen (oral) as directed on bottle Cough Drops for coughing, minor throat irritation as needed Antacid Tablet (oral) for stomach discomfort Benydryl (oral or topical) for swelling, hives, or allergic reaction as directed on bottle Calamine Lotion or Cortaid (topical) for insect bites/bee stings Visine/ Murine Plus Eye Drops (topical in eye) for minor eye irritation Other (please describe) ______________________________________________________ _________________________________________________________________________ PHYSICIAN CONSENT Physician Signature ______________________________________ Date ______________________ Printed Name __________________________________________ License Number ______________ Address ______________________________________________Phone _______________________ City _____________________________ State ________ Zip _______ Fax ______________________ This form must be turned in by June 1st . Duffield Summer Camps, 280 Warren Ave, Kenmore, NY, 14217 Rev.150116 Physician’s Report page 4 Camp Duffield Health Medication Forms Name of Camper: ___________________________________________DOB_____/_____/_____ For Prescription Medications: Any use of prescription drugs must be ordered by the Camper’s Physician and brought in original container. This form must be completed for each prescription to be administered and signed by the Camper’s Physician. For Over-the Counter Medications: Any additional over-the-counter medication not listed on above form must have specific directions and be in the original container. This form needs to be completed for these over-the-counter medication the Camper uses. Please give the following medications to the above named Camper: Name of Prescription Medication: ______ Dosage of Drug: Times to be administered: Length of time drug is to be given: Print Physician’s Name: Signature of Physician: Physician’s Phone No.: Date: Name of Over-the-Counter Medication: Dosage of the Drug: Times to be administered: Length of time drug is to be given: Signature of Parent/Guardian: This form must be turned in by June 1st . Duffield Summer Camps, 280 Warren Ave, Kenmore, NY, 14217 Rev.150116