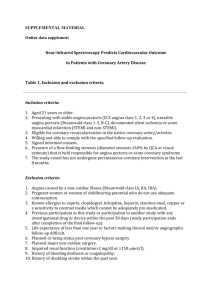
Online appendix. Methods Invasive treatment and clinical data
advertisement

Online appendix. Methods Invasive treatment and clinical data collection All STE-ACS patients were treated with aspirin (300 mg) and clopidogrel (600 mg) on admission to the Emergency Department. Percutaneous coronary interventions were performed through a radial or femoral access according to operator preference, using a 6 French catheter. A bolus of 5000 IU of heparin was administered. Glycoprotein IIb/IIIa inhibitors were administered after diagnostic angiogram at the start of percutaneous coronary interventions in all patients, as well as manual thrombus aspiration. All patients with NSTE-ACS received aspirin (250 mg IV loading dose, followed by aspirin 75 to 100 mg daily) and were treated with a loading dose of clopidogrel (600 mg) and fondaparinux or enoxaparin on admission to the Emergency Department. Use of IIb/IIIa inhibitors was left to operator’s decision. All patients with multivessel coronary artery disease without cardiogenic shock underwent PCI in nonculprit vessels with staged procedures before discharge following the index procedure. As a consequence, staged procedures were not taken in account for MACE rate. Patients with multivessel disease and cardiogenic shock were excluded from the study. In all patients cardiovascular risk factors were carefully examined, including family history of early coronary artery disease (first degree relative with a history of myocardial infarction <60 years), diabetes mellitus [fasting blood glucose >126 mg/dL or treated diabetes mellitus (intake of a diabetic diet or oral hypoglycaemic agents), according to the new ADA criteria (1)], hypercholesterolemia (total cholesterol >200 mg/dL or treated hypercholesterolemia), smoking (current), and hypertension (systolic blood pressure >140 mmHg and/or diastolic blood pressure >90 mmHg or treated hypertension). Body mass index was also obtained. Routine laboratory data, including full blood count, serum creatinine, glomerular filtration rate, glycaemia, lipid profile, fibrinogen and admission creatin-kinase and hs-Troponin T were also collected. Medications taken on admission were recorded. Finally, we acknowledge that 50 patients presenting with NSTE-ACS were also included in another report of our group (2). Collection of procedural and angiographic data 1 Coronary angiography was performed in two orthogonal projections using identical projection angles and table height throughout the entire procedure. Two expert angiographers (G.N. and H.R) evaluated off-line angiographic images both qualitatively and quantitatively (CAAS II; Pie Medical, Maastricht, The Netherlands). Lesion morphology was assessed using the modified American College of Cardiology/American Heart Association grading system (3), whereas coronary artery disease severity by counting the number of coronary artery branches showing at least one critical stenosis (≥70% reduction in lumen diameter), with multivessel disease defined as the presence of at least two-vessel disease. All measurements were performed on images obtained after intracoronary nitrate administration. The following quantitative angiographic parameters were obtained: reference vessel diameter, minimal lumen diameter and minimal diameter stenosis percent, which were evaluated both at baseline and at the end of the procedure, along with lesion length, total stent length/diameter and acute gain. All the analyses were performed inlesion with the exeption of reference vessel diameter that involved the segment containing the culprit lesion. OCT procedure Coronary angiography was performed via the transradial or transfemoral approach with the use of a 6F or 7F sheath. Unfractionated heparin (initial weight-adjusted intravenous bolus of 60 IU/Kg, with repeat boluses to achieve an activated clotting time of 250 to 300 seconds) was administered in all patients. The use of intracoronary or intravenous platelet IIb/IIIa inhibitors was left to the operators’ discretion in case of NSTE-ACS, while all STE-ACS patients received IIb/IIIa inhibitors. A 0.014-inch guidewire was placed distally in the target vessel and an intracoronary injection of 200 µg of nitroglycerin was performed. Frequency domain OCT (FD-OCT) images were acquired by a commercially available system (C7 System, LightLab Imaging Inc/ St Jude Medical, Westford, MA) connected to an OCT catheter (C7 Dragonfly; LightLab Imaging Inc/ St Jude Medical, Westford, MA), which was advanced to the culprit lesion. The FDOCT run was performed using the integrated automated pullback device at 20 mm/s. In case of STE-ACS patients, OCT was performed after vessel reopening with thrombus aspiration followed by gentle predilatation if necessary. In case of NSTE-ACS patients OCT was performed either directly or after gentle predilatation where OCT probe could cause a luminal obstruction. During image acquisition, coronary blood 2 flow was replaced by continuous flushing of contrast media directly from the guiding catheter at a rate of 4 ml/s with a power injector in order to create a virtually blood-free environment (4,5). OCT image analysis A thrombus was defined as an irregular mass protruding into the lumen or adjacent to the luminal surface. Thrombi were classified as red or white according to previous definitions (4,5). Tissue characteristics of underlying plaque were defined with previously established criteria (4,5). Plaques were classified as: 1) fibrous plaques (homogeneous, high backscattering areas); or 2) lipid-rich plaques (low-signal regions with diffuse border and with 2 or more lipid containing quadrants). Calcifications within plaques were identified by the presence of well-delineated, low back-scattering heterogeneous regions (4). Because red thrombi may reduce the ability to assess underlying structures because of the limited depth penetration of OCT laser light (≈1.5 mm) or the high backscattering with signal-free shadowing appearance, respectively, all OCT cross sections acquired within the coronary segment with thrombus were reviewed, one by one, for its entire longitudinal extension, for sites where vessel wall and plaque morphology could be assessed, as proposed in the expert document on OCT (4). Fibrous cap thickness in IFC was defined as the minimum distance from the coronary artery lumen to inner border of lipid pool, which was characterized by signal-poor region in OCT image. The thinnest part of the fibrous cap was measured 3 times, and the average value was calculated. For ruptured plaques the thinnest cap thickness was measured both at non-ruptured portion without communication between the lipid core and the lumen and at the thinnest part of the remnant of the disrupted fibrous cap. The thinnest cap thicknesses for each image were measured at two different times, and the average value was obtained. Minimum values, among the average values from each OCT image, were used for the analysis (6,7). Thincap fibroatheroma was defined as a plaque with lipid content in ≥2 quadrants and the thinnest part of a fibrous cap measuring ≤65 µm (5). Microchannels were defined as non-signal tubuloluminal structures without a connection to the vessel lumen, recognized on more than three consecutive cross-sectional OCT images (4). In the culprit segment the presence of thin-cap fibroatheromas other than the culprit lesion, calcifications and microchannels was assessed. Moreover, the length of calcified vessel was assessed as the sum of the 3 calcified plaque longitudinal lengths (mm) along the imaged vessel. The length of lipid vessel was assessed as the sum of the lipid plaque longitudinal lengths (mm) along the imaged vessel. The cross-section that had the highest quadrant number and the greatest arc of calcium or lipids was recorded together with the minimal fibrous cap thickness. Patients with coronary artery dissection or hematoma were excluded from the study. The OCT diagnosis of coronary artery dissection required the visualization of an intimomedial flap generating a double-lumen or an intramural hematoma. Intramural hematoma was considered when the intima was separated from the outer vessel wall by a relatively homogeneous material with high backscatter and variable attenuation (4,8). 4 References 1. American Diabetes Association. Standards of medical care for diabetes – 2014. Diabetes Care 2014;37:S14-S80. 2. Niccoli G, Montone RA, Cataneo L, Cosentino N, Gramegna M, Refaat H, Porto I, Burzotta F, Trani C, Leone AM, Severino A, Crea F. Morphological biohumoral correlations in acute coronary syndromes: pathogenic implications. Int J Cardiol 2014;171:463-466. 3. Ryan TJ, Bauman WB, Kennedy JW, Kreiakes DJ, King SB III, McCallister BD, Smith SC Jr, Ullyot DJ. Guidelines for percutaneous transluminal coronary angioplasty: a report of the ACC/AHA Task Force on Assessment of Diagnostic and Therapeutic Cardiovascular Procedures. J Am Coll Cardiol 1993;22:2033–5204. 4. Prati F, Regar E, Mintz GS, Arbustini E, Di Mario C, Jang IK, Akasaka T, Costa M, Guagliumi G, Grube E, Ozaki Y, Pinto F, Serruys PW; Expert's OCT Review Document. Expert review document on methodology, terminology, and clinical applications of optical coherence tomography: physical principles, methodology of image acquisition, and clinical application for assessment of coronary arteries and atherosclerosis. Eur Heart J 2010;31:401–415. 5. Tearney GJ, Regar E, Akasaka T, Adriaenssens T, Barlis P, Bezerra HG, Bouma B, Bruining N, Cho JM, Chowdhary S, Costa MA, de Silva R, Dijkstra J, Di Mario C, Dudek D, Falk E, Feldman MD, Fitzgerald P, Garcia-Garcia HM, Gonzalo N, Granada JF, Guagliumi G, Holm NR, Honda Y, Ikeno F, Kawasaki M, Kochman J, Koltowski L, Kubo T, Kume T, Kyono H, Lam CC, Lamouche G, Lee DP, Leon MB, Maehara A, Manfrini O, 5 Mintz GS, Mizuno K, Morel MA, Nadkarni S, Okura H, Otake H, Pietrasik A, Prati F, Räber L, Radu MD, Rieber J, Riga M, Rollins A, Rosenberg M, Sirbu V, Serruys PW, Shimada K, Shinke T, Shite J, Siegel E, Sonoda S, Suter M, Takarada S, Tanaka A, Terashima M, Thim T, Uemura S, Ughi GJ, van Beusekom HM, van der Steen AF, van Es GA, van Soest G, Virmani R, Waxman S, Weissman NJ, Weisz G; International Working Group for Intravascular Optical Coherence Tomography (IWG-IVOCT). Consensus standards for acquisition, measurement, and reporting of intravascular optical coherence tomography studies: a report from the International Working Group for Intravascular Optical Coherence Tomography Standardization and Validation. J Am Coll Cardiol 2012;59:1058-72. 6. Yonetsu T, Kakuta T, Lee T, et al. In vivo critical fibrous cap thickness for rupture-prone coronary plaques assessed by optical coherence tomography. Eur Heart J 2011;32:1251–9. 7. Tian J, Ren X, Vergallo R, Xing L, Yu H, Jia H, Soeda T, McNulty I, Hu S, Lee H, Yu B, Jang IK. Distinct morphological features of ruptured culprit plaque for acute coronary events compared to those with silent rupture and thin-cap fibroatheroma: a combined optical coherence tomography and intravascular ultrasound study. J Am Coll Cardiol 2014;63:220916. 8. Alfonso F, Canales E, Aleong G. Spontaneous coronary artery dissection: diagnosis by optical coherence tomography. Eur Heart J 2009;30:385. 6 Table 1 (Online appendix). Predictors of major adverse cardiac events at simple Cox regression analysis among clinical, angiographic and OCT characteristics. Variables HR 95% CI P Age 0.99 0.963-1.014 0.37 Male sex 0.895 0.445-1.80 0.755 Current smoking 1.24 0.795-1.942 0.34 Diabetes mellitus 1.115 0.542-2.294 0.77 Dyslipidaemia 1.44 0.741-2.784 0.28 Obesity (BMI>35) 1.898 0.970-3.715 0.06 Hypertension 1.04 0.507-2.126 0.92 Family history of CAD 1.63 0.859-3.092 0.135 Previous CAD 1.01 0.503-2.034 0.975 Previous ACS 1.30 0.599-2.829 0.51 Previous PCI 1.90 0.865-4.185 0.11 Previous CABG 1.83 0.248-13.480 0.55 Creatinine 0.97 0.629-1.497 0.89 TnT > 0.03 ng/mL 2.43 0.571-10.378 0.23 STE-ACS as clinical presentation 0.70 0.358-1.368 0.30 Statins 0.65 0.255-1.679 0.38 Culprit vessel 1.10 0.715-1.704 0.66 Multivessel disease 0.69 0.369-1.289 0.24 DES 1.405 0.748-2.639 0.29 DES type 1.22 0.541-3.871 0.42 Stent length 1.05 0.993-1.103 0.09 Stent diameter 0.96 0.578-1.580 0.86 B2/C lesion 0.97 0.477-1.673 0.73 RVD 0.98 0.887-1.211 0.88 MLD pre 0.89 0.482-1.782 0.77 DS% pre 0.79 0.551-1.314 0.43 MLD post 0.81 0.688-1.553 0.63 DS% post 1.03 0.891-1.322 0.76 Acute gain 1.05 0.790-1.224 0.79 Clinical variables Angiographic and procedural variables 7 OCT variables Culprit lesion analysis Plaque rupture 2.60 1.195-5.644 0.02 Lipid-rich plaque 1.74 0.726-4.158 0.215 Fibrous plaque 1.06 0.568-1.967 0.86 Calcified plaque 1.055 0.440-2.529 0.90 MLA 1.21 0.937-1.556 0.145 Cap thickness 1.00 0.986-1.008 0.58 Thrombus 0.77 0.393-1.508 0.445 Minimal cap thickness 0.99 0.982-1.007 0.36 TCFA 1.18 0.633-2.200 0.60 Presence of microvessels 0.915 0.486-1.723 0.78 Lipidic quadrants 1.02 0.829-1.262 0.83 Maximum lipid quadrant 1.03 0.785-1.348 0.84 Lipid arc degree 1.00 0.997-1.002 0.96 Maximum lipid arc 1.00 0.997-1.003 0.805 Lipidic length 1.00 0.995-1.006 0.79 Calcified length 1.00 0.994-1.008 0.76 Maximum calcium arc 1.00 0.997-1.005 0.505 Maximum calcium quadrant 1.11 0.807-1.537 0.51 Calcified nodules vessel 1.17 0.571-2.412 0.66 Culprit segment analysis Legend: ACS: acute coronary syndrome; BMI: body mass index; CABG: coronary artery by-pass graft; CAD: coronary artery disease; DES: drug-eluting stent; DS: diameter stenosis; MLA: minimal lumen area; MLD: minimal lumen diameter; PCI: percutaneous coronary intervention; RVD: reference vessel diameter; TCFA: thin-cap fibroatheroma. 8