Hepatitis E Virus Enhanced Surveillance
advertisement

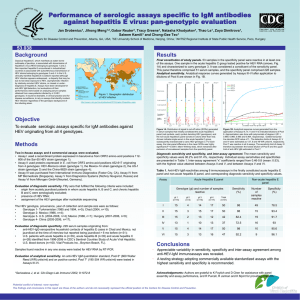
Hepatitis E Virus Enhanced Surveillance Hepatitis E virus epidemiology in England and Wales: Identifying risk factors for indigenous infection Study team Samreen Ijaz, Clinical Scientist, Virus Reference Department (VRD), HPA Colindale Bengü Said, Senior Scientist, Gastrointestinal, Emerging and Zoonotic Infections (GEZI) Department, HPA Colindale Meera Chand, Specialist Registrar, Medical Microbiology & Virology, HPA Colindale Dilys Morgan, Head, Gastrointestinal, Emerging and Zoonotic Infections Department, HPA Colindale Background Hepatitis E virus (HEV) infections in Europe and North America were believed to be associated with travel to endemic areas, however autochthonous hepatitis E has been increasingly recognised. Sequence analysis indicates that the genotype 3 HEV found in human infections in non-endemic countries is very similar to that found in swine and although contact with pigs and consumption of pig products have been reported as risk factors for some infections and outbreaks, a range of food sources and risk factors have been identified. 1,2 However, in most cases, the source of infection remains undetermined. Following the identification of non-travel associated cases of hepatitis E in England and Wales in 2004 3, enhanced surveillance was carried out in 2005 to identify potential risk factors for infections. That year saw a significant increase in the number of cases and 329 cases were confirmed of which 33 were established to be indigenous and a further 67 were likely to be indigenous infections. The majority were Caucasian males over 55 years of age, but a specific risk factor could not be identified.4 The number of confirmed cases dropped slightly in 2006 and significantly in 2007, but then started to increase again from 2008, showing a marked increase in 2010 (Table 1). Therefore it is felt that 1 routes of acquisition should be re-investigated in order to try and establish sources of infection and reduce the public health risk. Table 1: Cases of Hepatitis E infection confirmed by Reference Laboratories (Colindale and Birmingham) in England and Wales, 2005-2010. Year 2004 2005 2006 2007 2008 2009 2010 Number of confirmed cases 150 329 292 165 178 180 278 Aims and objectives Objective: To determine the possible risk factors for the acquisition of indigenous HEV infection in England and Wales. Our aim is for enhanced surveillance data to generate hypotheses on risk factors that can be tested in subsequent studies. Study Design and Methodology Period of study: Enhanced surveillance of hepatitis E cases of possible indigenous origin will commence June 2011. It will continue until a hypothesis has been generated or complete data has been gathered on a maximum of 25 non-travel-associated UK cases. This is estimated at 3 months. Design: Enhanced surveillance of cases diagnosed by reference laboratory. Cases for interview: HEV infection of possible indigenous origin will be identified using the following definition: A case that is confirmed by HPA Colindale VRD by (i) detection of HEV RNA OR (ii) detection of HEV IgG and IgM and has ‘no travel’ stated on the laboratory request form Or 2 if no travel information is given, patient is 50 years old or over with a Caucasian name 1 Or the virus is found to be genotype 3 through molecular characterisation Sample: Cases fulfilling the eligibility above will be contacted and interviewed until a maximum of 25 cases with full epidemiological information and no evidence of travel to endemic areas have been obtained. Methodology: (i) Surveillance procedure The regional hepatitis leads will be consulted regarding conducting enhanced surveillance. Information will be disseminated to Health Protection Units and Consultants in Communicable Disease Control. For cases diagnosed from June 2011 onwards, patient information will be passed securely from VRD to GEZI. GEZI will notify the appropriate Health Protection Unit. The protocol for obtaining surveillance information is shown in Figure 1. Either the HPU or GEZI will conduct a telephoneadministered questionnaire. All data will be entered into a secure Excel spreadsheet at HPA Colindale. (ii) Questionnaire The questionnaire has been developed following a review of literature on hepatitis E acquisition and using knowledge of transmission of other gastro-intestinal disease. Questions relating to demographic factors and possible risk factors are included. The main risk factors to be included are: Travel: Travel to an endemic area within the incubation period (in which case the interview will be terminated). For the Based on the previous study which found that being male, having a Caucasian name and being over 50 years was strongly predictive of being a non-travel related case 1 3 purposes of this study, countries in Africa and Asia will be considered endemic. Contacts: Known contact with people who have travelled to an endemic area. Food: Possibilities include pork, other meat products, shellfish and fresh vegetables. Water: Recreational water contact. Animals: Exposure to livestock, pets, or other animals. Sexual exposure: A question regarding sexual orientation and recent sexual partners is included. It is not felt to be appropriate to take a detailed sexual history in a telephone interview. As the incubation period of HEV varies between 2-9 weeks, gaining information about the exposure variables will be difficult. A trawling questionnaire will be used, asking open-ended question such as ‘Is it likely that you ate the following foods in the 9 weeks before onset of symptoms?’ Possible responses would be ‘yes, at home’, ‘yes, away from home’ and ‘never’ with an option to specify which type and source of food and if handled raw. If potential sources or routes of infection are identified, then the questionnaire will be modified for subsequent interviews to explore these factors. Rationale for design: Previous surveillance has not identified a route of acquisition for HEV in the UK. In view of the increase in cases in 2010, it is prudent to undertake detailed enhanced surveillance in order to gain more information about potential sources of infection and risk factors. Data Processing and Handling The data will be processed and handled by the study team in GEZI at HPA Colindale. A system is to be set up whereby data from the reference laboratory will be transferred in a timely way to GEZI so that cases can be promptly followed up. Data will be entered into Excel. Data Analysis 4 Data will be analysed using Excel. As this study involves hypothesis generation, analysis will predominantly be descriptive. Ethics Committee Approval Ethics Committee approval is not required for enhanced surveillance. Preferred timetable Critical stage Enhanced surveillance commenced Data collection completed Analysis completed Final report Date June 2011 September 2011 October 2011 November 2011 References 1 Lewis HC, Wichmann O, Duizer E. Transmission routes and risk factors for autochthonous hepatitis E virus infection in Europe: a systematic review. Epidemiol Infect. 2010;138 :145-66.. 2 Wilhelm BJ, Rajić A, Grieg J, et al. A systematic review/metaanalysis of primary research investigating swine, pork or pork products as a source of zoonotic hepatitis E virus. Epidemiol Infect. 2011 Apr 18:1-18. [Epub ahead of print] 3 Ijaz S, Arnold E, Banks M, Bendall RP, Cramp ME, Cunningham R et al. Non-travel-associated hepatitis E in England and Wales: demographic, clinical, and molecular epidemiological characteristics. J Infect Dis. 2005;192:1166-72. 4. Lewis HC, Boisson S, Ijaz S, Hewitt K, Ngui SL, Boxall E, et al. Hepatitis E in England and Wales. Emerg Infect Dis 2008; 14: 165-167 5 Figure 1: Process for enhance d surveilla nce of nontravelassociate d hepatitis E in England and Wales VRD receives sample for HEV testing Results compatible with or diagnostic of acute HEV infection* No evidence of acute HEV infection Request form: History of travel outside the UK Request form: ‘No travel’ stated or no travel information and Caucasian name and aged 50 years or over No further follow up Case data referred to HEV team HEV team contacts HPU to ask if they routinely interview hepatitis E cases If YES: send revised questionnaire to HPU for completion If NO: HPU does not agree to complete questionnaire Upload questionnaire to HPZone or email to zoonoses@hpa.org.uk or fax securely to 0208 905 9929 HEV team contacts patient and completes questionnaire 6 * A case that is confirmed by HPA Colindale VRD either by detection of HEV RNA (diagnostic of acute HEV infection) OR by detection of HEV IgG and IgM (compatible with acute HEV infection) 7