Physician Authorization Form - Lakeside Union School District
advertisement

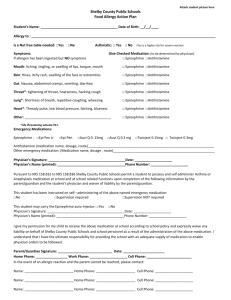
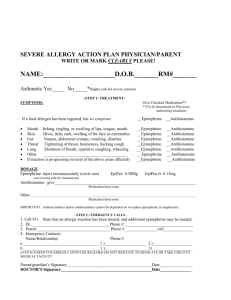
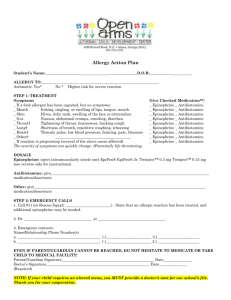
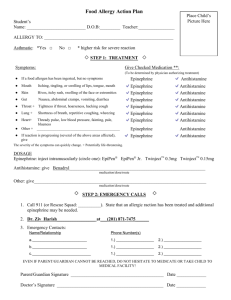
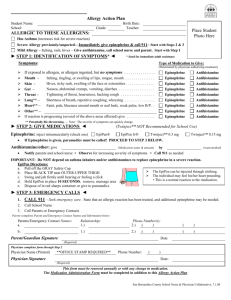
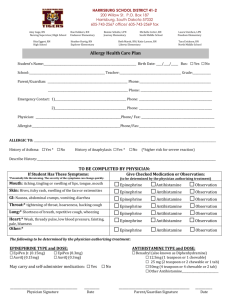
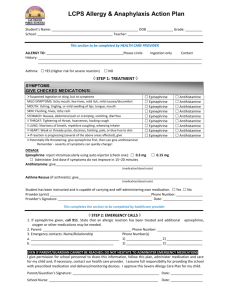
Lakeside Union School District Health Services Physician’s Authorization for Treatment of All Allergies Student: __________________________________________________ DOB: ________________ Teacher: __________________________________________________ School: ______________ A. To Be Completed By Parent/Guardian I hereby request that Lakeside Union School District, through its designated authority, supervise and or assist in the administering of medication to my child, according to the instructions contained on my physician’s statement below. I release the Board of Trustees, the school, and any employee from liability for administering any authorized medication. ___________________________________________________ Parent or Legal Guardian’s signature ____________________________________ ____________________ Phone# Date B. To Be Completed By Physician Only Allergy to: Life-Threatening? Yes Symptoms: No Treatment: Give checked Medication If a food allergen has been ingested, but no symptoms: Mouth Itching, tingling, or swelling of lips, tongue, mouth: Skin hives, itchy rash, swelling of face or extremities: Stomach- nausea, abdominal cramps, vomiting, diarrhea: Throat- tightening, hoarseness, hacking cough: Lung- Shortness of breath, repetitive coughing, wheezing: Heart- Weak or thready pulse, low blood pressure, fainting: Other: If reaction is progressing (several above areas affected) give: Epinephrine Epinephrine Epinephrine Epinephrine Epinephrine Epinephrine Epinephrine Epinephrine Epinephrine Antihistamine Antihistamine Antihistamine Antihistamine Antihistamine Antihistamine Antihistamine Antihistamine Antihistamine N/A N/A N/A N/A N/A N/A N/A N/A N/A Dosage: Epinephrine: inject intramuscularly according to above guidelines. (circle one) EpiPen 0.3mg EpiPen Jr. 0.15mg Twinject 0.3mg Twinject 0.15mg Antihistamine: give according to above guidelines. (medication, dose, route) . Other: (medication, dose, route) . Monitoring: Stay with student; alert EMS, parent, and District Nurse. Tell EMS epinephrine was given. Note time epinephrine was administered. A second dose of epinephrine can be given 5 min. or more after first dose if symptoms persist or recur. For a severe reaction, consider keeping student lying on back with legs raised. Treat student even if parents cannot be reached. **This form will need to be updated at the beginning of each school year** ________________________ ___________________ ______________ Printed name of physician Medical license number Telephone number ____________________________________ ____________________________ Physician Signature Date