Discharge Summary - Adaptive Geriatrics!
advertisement

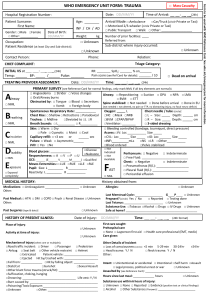
Adaptive Geriatrics Discharge Summary Insert facility address here (o) (804)xxx-xxxx (best number for families/providers to contact you) (f) (804)xxx-xxxx (best place to fax orders/notes) Patient Name: DOB: Date: Admitting Diagnoses: Rehab course: Admission date: ___/___/___ Projected D/C date: ___/___/___ PMSH: Medical: hospitalization Allergies: Important medication changes: *see med list for complete list of meds* Page 1 of 4 New Diagnoses since ROS: circle if positive, strike if negative KEY FINDINGS: Constitutional: Wt Loss, Wt Gain, Dizziness, Lightheadness, Fever, Chills, Lethargy Skin: Rash, Pruritus, Blister, Ulcer Eyes: Poor/Blurred Vision, Diplopia, Blindness, Glaucoma ENT: Hearing prob, Tinnitus, Runny nose, Sore throat, Difficulty chewing Resp: SOB, DOE, PND, Orthopnea, Wheezing, Cough, Tachypnea Sputum production CV: Chest pain, Tightness, Palpitations, Edema Breasts: Lumps/Masses, Nipple discharge GI: Loss of appetite, Pain, Dysphagia, Nausea, Vomiting, Diarrhea, Constipation, Melena, Hematemesis GU: Dysuria, Hematuria, Polyuria, Hesitancy, Frequency, Discharge, Vaginal bleeding, Pruritus Immuno/Allergies: Seasonal allergies, Joint pain, Swelling, Arthritis Endo: Polydipsia, Polyphagia, Heat/Cold intolerance Musculoskeletal: Joint pain, Swelling, Stiffness, Weakness, Parathesias, Speech Neuro: HA, Confusion, Seizures, Syncope, Numbness, Weakness, Paresthesias, Dysphasia, Memory loss Psych: Anxiety, Depression, Insomnia, Suicidal/Homicidal ideation PHYSICAL EXAM: (Check if normal, if abnormal write results) GEN: NAD Obese WD/WN CONST: T _______ BP _______ P _______ R ______ EYES: PERRLA Lids/Conjunctiva Nml Sclera Anicteric Nml Fundi ENT: NCAT Nml TMs/EACs Nml Nasal Mucosa/Turbinates Nml Oropharynx/Oral mucosa Nml Dentition/Gum NECK: Neck symmetrical and trachea midline Thyroid normal size with no masses RESP: Nml Effort Clear Bilat No tactile fremitus or crepitus palpated No Hyperessonance or dullness CV: No JVD No Bruits Regular Rate No Rubs ABD: Nondisplaced PMI Regular Rhythm Flat Nontender Nondistended No Masses Nml Rectal Tone GU: Male: Nml Testes Female: LYMPH: MK: Soft No Hernia No Hemorrhoids No Discharge No Vaginal discharge No Nipple discharge No Adenopathy in two or more regions Nml gait and station No Deformity No Contractures No clubbing or cyanosis of nails Nml muscle tone Page 2 of 4 Obese No Skin changes No Spinal tenderness SKIN: Nml DP/PT Pulses No Penile Lesions No Masses No Gallops No Hepatosplenomegaly Nml External Genitalia BREASTS: Nml S1 S2 No Peripheral Edema Nml Bowel Sounds No Murmurs No Rash Nml ROM No Ulcers No Active synovitis No Subluxation Nml strength No nodules or induration Poor Historian due to: All other ROS negative KEY FINDINGS: Neuro: Alert Nml DTR’s Psych: Oriented CN 2-12 Intact Absent tremor Nml Light Touch No Abnormal movements Nml Mood/Affect Mental Status: Unchanged from baseline See attached BIMS Functional Status: Indicate level as follows: 1= Independent:; 2= uses adaptive device; 3= help from others; 4= totally dependent: Ambulation: ___ Toileting: ___ Nutrition: Weight: _____ stable Diet: No restrictions Eating: ___ Transfers: ___ Ability to position in bed:_ __ increase decrease of ____ pounds over ___ months Special diet/consistency: __________________________________ PERTINENT LAB DATA/TEST RESULTS: Follow up: Please make a follow up appointment with your primary care doctor within 2 weeks of discharge You should have the following blood work done: Please have your doctor check: ________________________________________ in __________ days/weeks ________________________________________ in __________ days/weeks You should have the following tests done: Please have your doctor schedule a ___________________________ in ______ days/weeks You should see the following specialists within 2 weeks of discharge: ______________________________ Discharge Diagnoses/Follow up plans: > 30 minutes spent in discharge summary Signature: __________________ Signature: __________________ Signature: ___________________ Your Name, Credentials Provider you work with Provider you work with Page 3 of 4 Discharge Medication List/Prescription Your Name DEA #: xx123456 NPI#: 1234567 Facility Address (o) (804)XXX-XXXX (best number for pharmacist to call) (f) (804)xxx-xxxx (best place to fax orders) Patient Name: _________________________________________ Call these meds in Medication and dose Instructions for administration Date: _____________ Dispense # Refills Brand Medically Necessary Voluntary Formulary Permitted: _______________________________________ Your Name, Credentials *IN ORDER TO BE VALID, THIS FORM MUST BE CALLED IN TO THE PHARMACY FROM THE NURSING FACILITY* Page 4 of 4

![Natural_Moral_Law_part_2[1]](http://s2.studylib.net/store/data/005436322_1-5343ff09fdfd6d3656ebca597d8369e8-300x300.png)