Dig Toxicity
advertisement

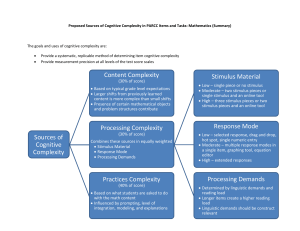
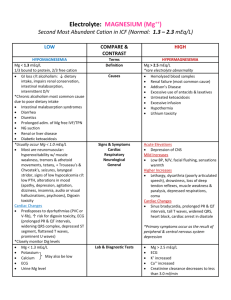
For Examiner Only Case Digoxin Toxicity Author Emily Goren, MD Reviewer Francis DeRoos, MD Approved: 12/28/05 ORAL CASE SUMMARY CONTENT AREA Toxicology SYNOPSIS OF CASE Chronic digoxin toxicity with hypotension and bradycardia requiring treatment with digoxin specific FAB fragments (Digibind). SYNOPSIS OF HISTORY 80 year-old female complaining of progressive nausea and vomiting for 3 days. She complains of generalized abdominal cramping and generalized weakness. SYNOPSIS OF PHYSICAL Elderly female weak and vomiting with bradycardia. CRITICAL ACTIONS 1. Recognizes and immediately addresses unstable vitals, ordering IV access, Oxygen, and Monitoring. 2. Addresses hypotensive bradycardia ordering IVF. (PM) 3. Takes complete history including medications (digoxin). (DA) 4. Correctly interprets EKG: recognizes complete av block, junctional bradycardia, ST changes. (PS) 5. Administers Digibind. (PS) (PM) 6. Discusses diagnosis and treatment plan with patient. (IR) 7. SCORING GUIDELINES (Critical Action No.) Score down if the candidate fials to initiate resuscitation and order an ECG. Penalize if medication history and digoxin use isn’t noted. Score down if candiate fails to appreciate digoxin toxicity on the ECG and needs to be prompted FOR EXAMINER ONLY For Examiner Only PLAY OF CASE GUIDELINES (Critical Action No.) • Case diagnosis is chronic digoxin toxicity. • Patient is hypotensive and bradycardic. • Candidate orders IV, monitor, and oxygen. • Candidate takes history including medications (digoxin). • Candidate performs focused physical exam. • Candidate orders appropriate labs, and EKG which demonstrates complete av block with junctional escape and characteristic ST changes. Digoxin level should be ordered after EKG, if not done initially. • Candidate orders IV fluid – no success. • Repeat vitals reveal worsening bradycardia and hypotension. Candidate orders atropine – no success. • Candidate may order pressors, attempt transcutaneous pacing or transvenous pacing – no success. • Digoxin level is 4. • Candidate treats digoxin toxicity with Digibind. Calculated dose for chronic toxicity is level x weight in Kg / 100. Here patient is 50kg x 4 / 100 = 2 vials. • Candidate contacts patient’s primary doctor and admits to ICU. • Patient’s heart rate and blood pressure improve. Repeat EKG shows sinus rhythm with first degree av block. • Candidate discusses diagnosis and treatment plan with patient.. FOR EXAMINER ONLY For Examiner Only Critical Actions 1. Recognizes and immediately addresses unstable vitals, ordering IV access, Oxygen, and Monitoring. This critical action is met by recognizing and immediately addressing unstable vitals, ordering IV, Oxygen, and Monitoring. (PS) Cueing Guideline: Nurse asks if there are any orders. 2. Addresses hypotensive bradycardia ordering IVF. (PM) This critical action is met by addressing hypotensive bradycardia ordering IVF. (PM). Cueing Guideline: Patient complains of feeling dizzy. Vital signs worsen. 3. Takes complete history including medications (digoxin). (DA) This critical action is met by taking complete history including medications (digoxin). (DA) Cueing Guideline: Nurse is going through patient’s belongings and asks if you want to see patient’s pill bottles. 4. Correctly interprets EKG: recognizes complete av block, junctional bradycardia, ST changes. (PS) This critical action is met by correctly interpreting EKG: recognizes complete av block, junctional bradycardia, ST changes. (PS) Cueing Guideline: Nurse asks what the EKG shows. 5. Administers Digibind. (PS) (PM) This critical action is met by administering Digibind. (PS) (PM) Cueing Guideline: Nurse asks if you have any medication orders. Patient does not respond to any other intervention e.g. atropine, pressors, pacing. 6. Discusses diagnosis and treatment plan with patient. (IR) This critical action is met by discussing diagnosis and treatment plan with patient. (IR) Cueing Guideline: Patient starts crying – she wants to know what is going to happen to her. For Examiner Only Case Digoxin Toxicity History Data Panel Age: 80 Sex: Female Name: Velma Vixen Method of Transportation: Daughter Person giving information: Patient Presenting complaint: Vomiting for 3 days Onset and Description of Complaint: Patient complains of progressive nausea and vomiting for 3 days. She complains of generalized abdominal cramping and generalized weakness. (-) fever. (+) chills. (-) diarrhea, melena or hematochezia. She denies chest pain and shortness of breath. Past Medical History Allergies: PCN Medical: CHF, HTN, NIDDM, gastritis, hypothyroidism, glaucoma Medications: Altace (ramipril) 5 mg BID Lasix (furosemide) 40 mg QD Glucotrol 5 mg QD Lanoxin (digoxin) 0.25 mg QD Tagamet (cimetidine) 300 mg QHS Levoxyl (levothyroxine) 100 mcg QD Alphagan drops 0.2% OU BID Surgical: Hysterectomy Last Meal: Few crackers yesterday Habits Smoking: None. Drugs: Denies. Alcohol: Denies. Family Medical History Father: NC Mother: NC Siblings: NC Social History Married: Widowed Children: 2 Employed: Retired school teacher Education: College PMD: Sally Bright, MD For Examiner Only Case Digoxin Toxicity Physical Data Panel General Appearance: Pale, elderly female who appears weak, vomiting in bed. Vital Signs: BP : P : R : T : O2Sat : Glucose : 85/40 46 20 96.9 96% on RA 250 Repeat: 70/30 28 24 After Digibind: 135/80 70 20 Neurological: CN II-XII intact. No focal motor or sensory deficits. Mental Status: Alert and Oriented x 3. Head: NCAT. Eyes: PERRL, EOMI. Ears: Normal. Mouth: Mucous membranes dry and pale, OP clear. Neck: Supple, no LAD, no JVD. Skin: Dry and pale. Chest: Slight tachypnea. Lungs clear to auscultation and equal bilaterally. Heart: Normal S1 / S2. Bradycardia. No murmurs, rubs or gallops. Abdomen: NABS. Soft, non-distended. Mild diffuse tenderness greatest in lower quadrants bilaterally. No masses. Extremities: No clubbing, cyanosis, or edema. Rectal: Brown stool, Guiac negative. Pelvic: Patient refuses. Back: Kyphoscoliosis. No CVA tenderness. Other exam findings: For Examiner Only Case Digoxin Toxicity Lab Data Panel Stimulus #2 – CBC WBC Hgb Hct Platelets Differential Segs Lymphs Monos Eos 14.7/mm3 9.1 g/dL % 358 /mm3 86% 12% 2% 1% Stimulus #5 – Liver Enzymes and Lipase Normal Stimulus #6 – Digoxin Level 4.0 ng/mL (0.5 - 1.5 ng/mL) Stimulus #7 – EKG: Complete av block with junctional escape, characteristic ST depressions Stimulus #8 – Portable CXR: Negative Stimulus #3 – Chemistry Na+ 133 mEq/L K+ 3.8 mEq/L HCO322 mEq/L Cl99 mEq/L Glucose 227 mg/dL BUN 38 mg/dL Creatinine 1.4 mg/dL Stimulus #4 – Coagulation Panel PT 12 PTT 24 Stimulus #9 – EKG after treatment: Sinus with 1st degree av block VERBAL REPORTS Rhythym strip Accucheck AV block in 40's 250 For Examiner Only Case Digoxin Toxicity Stimulus Inventory Stimulus #1 – Emergency Admitting Form Stimulus #2 – CBC Stimulus #3 – Chemistry Stimulus #4 – Coagulation Panel Stimulus #5 – Liver Enzymes and Lipase Stimulus #6 – Digoxin Level 4.0 ng/mL (0.5 - 1.5 ng/mL) Stimulus #7 – EKG: Complete av block with junctional escape, characteristic ST depressions Stimulus #8 – Portable CXR Negative Stimulus #9 – EKG after treatment: Sinus with 1st degree av block FOR EXAMINER ONLY Mock Oral Feedback Form – ABEM model Case Digoxin Toxicity Date: Examiner: Examinee: Data acquisition Worst 1 NOTES 2 3 4 5 6 7 8 Best Problem solving Worst 1 NOTES 2 3 4 5 6 7 8 Best Patient management Worst 1 2 NOTES 3 4 5 6 7 8 Best Resource utilization Worst 1 2 NOTES 3 4 5 6 7 8 Best Health care provided Worst 1 2 NOTES 3 4 5 6 7 8 Best 4 5 6 7 8 Best Comprehension of path physiology Worst 1 2 3 4 NOTES 5 6 7 8 Best Clinical competence (overall) Worst 1 2 3 NOTES 5 6 7 8 Best Patient Interpersonal relations Worst 1 2 3 NOTES 4 Critical Actions Dangerous actions 1. Recognizes and immediately addresses unstable vitals, ordering IV access, Oxygen, and Monitoring. 2. Addresses hypotensive bradycardia ordering IVF. (PM) and omissions fials to initiate resuscitation and 3. Takes complete history including medications (digoxin). (DA) 4. Correctly interprets EKG: recognizes complete av block, junctional bradycardia, ST changes. (PS) 5. Administers Digibind. (PS) (PM) order an ECG. Penalize if 6. Discusses diagnosis and treatment plan with patient. (IR) FOR EXAMINER ONLY Score down if the candidate medication history and digoxin use isn’t noted. Score down if candiate fails to appreciate digoxin toxicity on the ECG and needs to be prompted Mock Oral Feedback Form – Core Competencies Case Digoxin Toxicity Date: Examiner: Does not meet expectations Examinee: Meets Expectations Exceeds Expectations 1. Patient care 2. Medical knowledge 3. Interpersonal skills and communication 4. Professionalism 5. Practice-based learning and improvement 6. Systems-based practice Critical Actions Dangerous actions 1. Recognizes and immediately addresses unstable vitals, ordering IV access, Oxygen, and Monitoring. 2. Addresses hypotensive bradycardia ordering IVF. (PM) and omissions fials to initiate resuscitation and 3. Takes complete history including medications (digoxin). (DA) 4. Correctly interprets EKG: recognizes complete av block, junctional bradycardia, ST changes. (PS) 5. Administers Digibind. (PS) (PM) order an ECG. Penalize if 6. Discusses diagnosis and treatment plan with patient. (IR) FOR EXAMINER ONLY Score down if the candidate medication history and digoxin use isn’t noted. Score down if candiate fails to appreciate digoxin toxicity on the ECG and needs to be prompted Stimulus #1 ABEM General Hospital Emergency Admitting Form Name : Velma Vixen Age : 80 Sex : Female Method of Transportation : Daughter Person giving information : Patient Presenting complaint : Vomiting for 3 days Background: Velma Vixen, an 80 yo female presents to ED complaining of vomiting for 3 days. Vital Signs Vital Signs: T 96.9 P 46 RR 20 BP 85/40 Stimulus #2 – CBC WBC Hgb Hct Platelets Differential Segs Lymphs Monos Eos 14.7/mm3 9.1 g/dL % 358 /mm3 86% 12% 2% 1% Stimulus #3 – Chemistry Na+ 133 mEq/L K+ 3.8 mEq/L HCO322 mEq/L Cl99 mEq/L Glucose 227 mg/dL BUN 38 mg/dL Creatinine 1.4 mg/dL Stimulus #4 – Coagulation Panel PT 12 PTT 24 Stimulus #5 – Liver Enzymes and Lipase Normal Stimulus #6 – Digoxin Level 4.0 ng/ml (0.5-1.5 ng/ml) Stimulus #7 – EKG Stimulus #8 – CXR Stimulus #9 – EKG after Treatment