Physical Therapy Protocol
advertisement

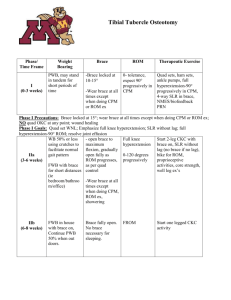
Brooke Army Medical Center Sports Medicine Outpatient Rehabilitation Protocol Anterior Cruciate Ligament Reconstruction Bone Tendon Bone (BTB) & Hamstring (Quad HS) Graft Reconstructions BAMC Ortho: 210-916-1242 BAMC PT: 210-916-1920 This Rehab Protocol is a guideline. Specific exercises and time frames may be altered depending on patient progression except italicized and bolded items. INPATIENT: Post-operative day (POD) 1 through discharge (d/c) from hospital PT Sessions: Morning and afternoon sessions each day Ambulation: Crutches – Progressive weight-bearing as tolerated (WBAT) Brace: 1. 2. 3. Knee immobilizer or hinged range-of-motion (ROM) brace Wear at all times while in bed (maintain full extension) Ambulate in locked ROM brace Remove knee immobilizer or ROM brace for rehabilitation exercises Exercise: 1. 2. 3. Calf / ankle pumps Static quad sets or straight leg raises (SLR) in full extension Assisted heel slides Inpatient DC Goals: 1. Full Extension 2. Good quadriceps contraction 3. Independent in WBAT ambulation with crutches 4. Patient demonstrates understanding of positioning & effusion control, cryotherapy at least 3 x day indep with home use 5. Outpatient therapy appointment coordinated by house ortho staff PHASE I: Hospital d/c through Week 4 – PROTECTION AND PAIN/EFFUSION CONTROL PT Sessions: 3-5 supervised sessions per week with outpatient physical therapist Ambulation: Crutches –WBAT; d/c when satisfactory quad strength (30 SLRs w/o lag) and normal gait. Brace: Wear at night for 6 weeks Discontinued during gait when quad strength is good and gait is normal. Exercise: 1. ROM: a. Bike (in available range. Should not be painful.) b. Patella mobilization (emphasize superior glides) c. PROM, AAROM, AROM as tolerated i. Heel slides (AAROM/PROM w/ HS graft) ii. Supine extension on bolster or prone hang 2. OKC strengthening: a. SLR x 4 on mat – add light ankle weights if quad control is maintained (less or no resistance for ADD) b. Electrical stimulation (PRN) in full extension with quad sets and SLR. Biofeedback when patient demonstrates good quad contraction c. HS isometrics. Progress to curls (prone or standing) for BTB only d. No resisted OKC extension 0-30 deg x 6 mo 3. CKC strengthening a. wall squats b. Total Gym – progress levels of mini-squats as tolerated c. Forward, lateral, and retro step downs in parallel bars -no knee flexion past 30 degrees d. Bilateral heel raises. Progress to single leg as tolerated 4. Scar massage when incision healed 5. Gait training 6. Proprioceptive training a. Wt shift to single leg stance 7. Ice x 15-20 minutes in full extension after each exercise session. Monitor effusion and pain carefully Goals and Criteria for Progression to PHASE II: 1. Full passive and active ROM and good patella mobility (Flexion to 90 by 1 wk, 110 by 2wks, 120 by 4 wks, full flexion AROM by 6wks; Extension equal to opposite side by 2 weeks) 2. Good quad control (No extensor lag; biofeedback to 80% vs. uninvolved side; >2 cm superior patella glide w/ quad set) 3. Single leg stance x 30 seconds, eyes open 4. Pain under control and minimal effusion 5. Normal gait without crutches PHASE II: Week 4 through Week 12 – STRENGTHENING PHASE PT Sessions: 3 supervised sessions per week with outpatient physical therapist Ambulation: Crutches should be discontinued Brace: none required Exercise: 1. 2. 3. 4. 5. 6. 7. Patellar mobilization, AROM, PROM with end-range stretching as needed OKC strengthening a. Initiate Hamstring curls, standing or prone, for hamstring grafts as tolerated b. No resisted OKC extension 0-30 deg x 6 mo c. Week 6: Start isokinetic quadriceps exercises 90-40 deg (180/300 /sec) CKC strengthening a. Standing 4-way hip strengthening b. Single leg press; single leg total gym mini squats c. Single leg wall squat d. Step ups e. Lunges Continue scar massage Initiate cardiovascular exercise stationary bike (when range at least 0-110) treadmill walking – forward and backward Proprioception drills: a. single leg body blade, ball toss, foam pad, etc. b. BAPS board c. Wobble board Aquatic (pool) therapy a. pool walking – forward and lateral b. flutter kicks (knee remains extended) c. weightless jogging d. Pool plyometric program at 8 weeks Goals and Criteria for Progression to PHASE III: 1. Full AROM 2. Normal quad and HS control 3. Single leg stance x 30 sec, eyes closed 4. Minimal pain; no effusion 5. Normal patellar mobility PHASE III: Week 12 through Week 18 – ADVANCED STRENGTHENING PHASE: PT sessions: Necessity of supervised sessions to be determined by physical therapist. If good ROM and muscle control, may progress to independent rehab program. Exercise: 1. 2. 3. 4. 5. Progress with PHASE II exercises Functional activities a. Fitter b. Lateral walking c. Figure 8s Cardiovascular exercise: a. Elliptical trainer, bicycle, swimming b. No running until 4 months or until passing isokinetic strength test (> 80%). No fast cutting, twisting or contact sports until 6 months or until phase IV goals met. No resisted OKC extension 0-30 deg x 6 mo Advanced pool therapy a. Treading water b. Kickboard swimming c. Pool running, shuffling, and carioca d. Modified aquatic sports Biodex Isokinetic Strength Test at 12 – 16 weeks blocked from 0-30 Goals and Criteria for Progression to PHASE IV: 1. No pain or swelling 2. No giving-way 3. Walk 3 miles at 15 min/mile pace 4. Isokinetic testing 80% vs. uninvolved side PHASE IV: Week 18 through Week 24 –BASIC FUNCTIONAL TRAINING: PT sessions: Necessity of supervised sessions to be determined by physical therapist. If good ROM and muscle control, may progress to independent rehab program. Optional: Biodex Isokinetic Strength Test at 20-24 weeks blocked from 0-10 Functional Tests: 1. Single leg hop for distance 2. Timed 6 meter hop 3. Triple hop for distance 4. Crossover: 3 controlled hops, measure for distance and time Exercises: 1. 2. 3. Continue with PHASE III exercises with increasing weight/intensity Progressive agility and proprioception exercises Begin impact activities (running, plyometrics) 4. No resisted OKC extension 0-30 deg x 6 mo Goals and Criteria for Progression to PHASE V: 1. No pain or swelling 2. Slow, controlled, alternating gait up and down stairs 3. Functional tests 85% uninvolved side 4. Isokinetic tests 90% of uninvolved side, if performed PHASE V: 6 Months + -- ADVANCED FUNCTIONAL TRAINING PT sessions: Supervised sessions to be determined by outpatient physical therapist. Minimum monthly follow-up visit if patient has HEP. Exercises: 1. 2. 3. 4. 5. 6. 7. Continue with PHASE IV exercises with increasing weight and difficulty Plyometrics Jumping / hopping progression Running progression Functional hop test as appropriate when running is normal Functional progression to cutting and jumping Return to sports prn when full strength and agility achieved Goals: Return to full duty and sport if (Low-profile ACL sports brace when required by surgeon): 1. Functional tests 85% of uninvolved side 2. Isometric tests 90% of uninvolved side, if performed 3. No pain or effusion 4. Full ROM 5. MD approval _____________________ David R. Brown, MD LTC, MC Orthopedics _________________________ KATHLEEN S. ZURAWEL, PT, OCS COL, SP Chief, Physical Therapy APPROVE / DISAPPROVE APPROVE / DISAPPROVE Updated 19 July 2006