Computer Library Project
advertisement

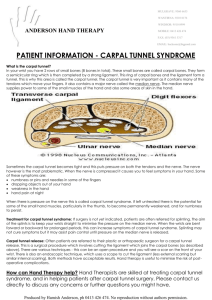
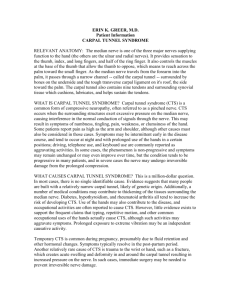
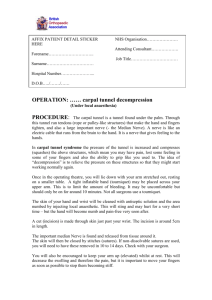
Mackenzie Morris PT 100 Library Project Fall 2013 Carpal Tunnel Carpal Tunnel Syndrome is the most commonly reported entrapment neuropathy of the upper limbs (1). It mainly affects workers, employers, and their insurers (1). It impacts employers because of lost work time, lost productivity, and the costs of treatment for carpal tunnel (2). The cause of carpal tunnel is similar for all workers, but symptoms and treatment methods can be different from worker to worker. The main cause of carpal tunnel is when too much pressure is placed on the median nerve that runs through the wrist (3). Pressure on the median nerve occurs because the transverse carpal ligament and the carpal bones, which form the carpal tunnel where the nerve passes through, has very little give (3). The transverse carpal ligament can become thick from wear and tear of the aging process or repetitive motion. The thickness then causes the nerve to be pressed against the tunnel (3). The pressure causes pain and symptoms which then leads to the diagnosis of carpal tunnel. Carpal tunnel has a lot of symptoms that affects workers. Many workers report pain and sensory disturbances, diminished hand function, and sleep problems (2). Early on in Carpal Tunnel Syndrome, patients will describe the feeling of their hands going to sleep. They also say that there is a lot of stiffness or weakness in their hands when they use them. Eventually, there will be a lot of pain which interrupts sleep and is noticed when they wake up. The pain will then also be present when they are doing common things like driving, holding a phone, or reading a References: 1, 2, 3 book. If patients grips something for a long time, symptoms will become stronger than they were but stop when patients release their grip. The pain that they feel can be different for each person. It often occurs in fingers one through four, the palm, and the forearm. For some patients, the pain will radiate to their shoulder which leads to a wrong assumption of what is happening (5). If patients visit a doctor, they will be given the diagnoses of carpal tunnel and then given a treatment plan depending on their symptoms. Treatment plans for carpal tunnel are all different depending on the situation. There are still many controversies regarding the treatments that are used for carpal tunnel and being able to prove scientific evidence that the treatment works (2). Regardless of the controversies, most patients are referred to either surgical treatment or non-surgical treatments depending on their symptoms (5). Surgical treatment is for patients who have persistent carpal tunnel symptoms and a lot of sensory disturbance, and non-surgical treatment is for mild to moderate symptoms (4). If a patient is referred to surgery, the doctor will divide the transverse carpal ligament which will open up the carpal tunnel and relieve the pressure (3). Most often patients then go to therapy after the surgery and complete a treatment plan like a patient would do for non-surgical treatment. The most common therapies used are splinting, exercise or mobilization, therapeutic ultrasound and oral medication (4). All of these treatments can vary in intensity and depend on the severity of the carpal tunnel (4). Carpal tunnel is a common problem in workers. Their symptoms affect their daily life and can cause a lot of frustration with workers and employers. As research on treatments for carpal tunnel is growing, more effective treatments and preventions are being used. Carpal tunnel is a common and painful syndrome which is why it is the most commonly reported entrapment neuropathy of the upper limbs. References: 2, 3, 4, 5 References 1. Burt S, Deddens JA, Crombie K, Jin Y, Wurzelbacher S, Ramsey J. A prospective study of carpal tunnel syndrome: workplace and individual risk factors. Occup Environ Med. 2013 Aug; 70(8):568-74. Epub 2013 Jun 20. 2. Groth G. Predicting intentions to use research evidence for carpal tunnel syndrome treatment decisions among certified hand therapists. Journal Of Occupational Rehabilitation. December 2011;21(4):559-572. Available from: CINAHL, Ipswich, MA. Accessed October 20, 2013. 3. Hertfelder SD, Gwin CH, Jackson LL. Hand/Orthotics. Bethesda, MD: The American Occupational Therapy Association, Inc.; 1995. 4. Page MJ, O’connor D, Pitt V, Massy-Westropp N. "Exercise and mobilisation interventions for carpal tunnel syndrome". Cochrane database of systematic reviews 2012, Issue 6. Art. NO.: CD009899. 5. Rosenbaum RB, Ochoa JL. Carpal Tunnel Syndrome and Other Disorders of the Median Nerve. 2nd ed. Woburn, MA: Butterworth-Heinemann; 2002.