DOCX ENG

H- 06 : cancers of the kidney
H-15 : cancers
When should children surviving a Wilms tumor be transplanted?
Uwe Querfeld & Constantinos J. Stefanidis
Nature Reviews Nephrology 8, 443-444 (August 2012)
ABSTRACT
Although children with Wilms tumor now have excellent survival rates, some develop endstage renal disease (ESRD) owing to immediate nephrectomy or later loss of renal function.
According to current recommendations, renal transplantation should be delayed for 2 years following Wilms tumor treatment in children, but data from the National Wilms Tumor Study now question such a waiting period.
COMMENTS
Wilms tumor (WT) is the most common childhood abdominal malignancy, with an incidence of approximately one in 10,000 newborns. The prognosis of children with WT has improved dramatically over the past three decades, with multidisciplinary therapeutic approaches leading to survival rates approaching 90% in children with localized disease and over 70% in those with metastatic disease.
Children who survive WT treatment are at risk of impaired renal function, however, primarily related to nephrectomy, surgery reducing the renal mass, radiation to the remaining kidney(s), nephrotoxic chemotherapy (such as ifosphamide and carboplatin) or genetic conditions.
An analysis of data from the National Wilms Tumor Study (NWTS) Group and the US Renal
Data System (USRDS) showed that patients at highest risk of developing end-stage renal disease (ESRD) had a constitutional mutation or deletion of the tumor suppressor gene WT1.
The consensus is that children with ESRD should receive a kidney transplant as soon as possible. For those with WT, however, current European guidelines for renal transplantation recommend a 2-year waiting period following WT treatment8 because the majority of tumor relapses occur during this time. Survival after recurrence of WT is only in the 50 –60% range.
Concern exists that a rule of delaying transplantation for 2 years may preclude transplantation for the large number of patients who never experience such complications — only 10 –15% of individuals with WT experience recurrence.
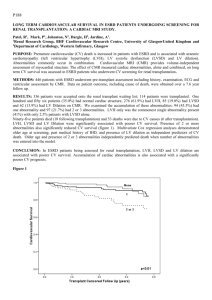
Recent data originating from the NWTS have provided new insights into the question of the safety of renal transplantation in patients with WT.Among a study population of 9,162 individuals diagnosed with a WT before the age of 15 years, the researchers identified 173 patients who had received dialysis or a renal transplant for treatment of ESRD. The authors compared clinical course, risk of tumor recurrence and patient and transplant survival in two patient groups defined by whether ESRD onset was categorized as being due to progressive bilateral WT (PBWT; n = 55) or to chronic kidney disease (CKD; n = 118). ESRD was
determined to be due to PBWT if it occurred at the time of surgical removal of all kidney tissue as a consequence of PBWT, and it was categorized as being due to CKD if it occurred in patients with unilateral WT or with bilateral WT in complete remission for at least 1 year.
Patient survival was markedly different between the groups (44% in the PBWT group versus
73% in the CKD group at 10 years). This difference was largely caused by increased rates of early death related to the malignancy or to chemotherapy in PBWT group patients, who were much younger at onset of ESRD than were patients in the CKD group (median age 4 years versus 15 years, respectively).
This study has opened the door for considering a review of the 2-year wait rule for renal transplantation after WT. Patients with a low-risk WT who remain relapse-free for 6 months after treatment might be considered for transplantation.
Pr. Jacques CHANARD
Professor of Nephrology