WHAT Is ANTHROPOMETRY 1
advertisement

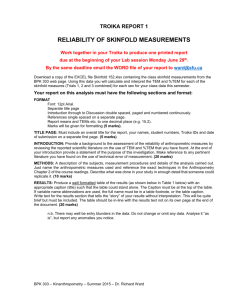
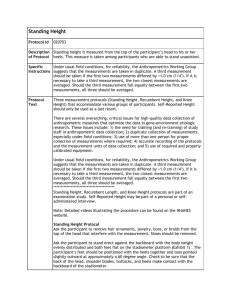
no 3 Methods Of Nutritional Assessment 1- Anthropometric Measurements WHAT IS ANTHROPOMETRY? Anthropometry is the measurement of body size, weight, and proportions. Measures obtained from anthropometry can be sensitive indicators of health, development, and growth in infants and children. Anthropometric measures can be used to evaluate nutritional status, whether it be obesity caused by over nutrition or emaciation resulting from protein-energy malnutrition. They are valuable in monitoring the effects of nutritional intervention for disease, trauma, surgery, or malnutrition. Anthropometry also is considered the method of choice for estimating body composition in a clinical setting. MEASURING LENGTH, STATURE, AND HEAD CIRCUMFERENCE • Measurements of length, stature (or height), weight, and head circumference are among the most fundamental and easily obtained anthropometric measurements. Among infants and children, these measurements are the most sensitive and commonly used indicators of health. • A child’s growth and development can be assessed by comparing height for age, weight for age, weight for height, and BMI for age with standards obtained from studies of large numbers of healthy, normal children. 1 • The measurement of stature is important for calculating certain indices such as weight for stature, weight divided by stature, and for estimating basal energy expenditure. • In measurements of length and stature, reference will be made to positioning the head in the Frankfort horizontal plane. As shown below, this plane is represented by a line between the lowest point on the margin of the orbit (the bony socket of the eye) and the tragion (the notch above the tragus, the cartilaginous projection just anterior to the external opening of the ear). With the head in line with the spine, this plane should be horizontal. Length • Length (also referred to as recumbent (horizontal) length) is obtained with the subject lying down and generally is reserved for children less than 24 months of age or for children between 24 and 36 months of age who cannot stand erectly without assistance. • The growth charts used for persons birth to 36 months of age are based on recumbent length, whereas the growth charts for those age 2 to 20 years are based on stature. • Measurement of recumbent length requires a special measuring device with a stationary headboard and moveable foot- board that are perpendicular to the backboard. The device’s measuring scale (in millimeters or inches) should have its zero end at the edge of the headboard and allow the child’s length to be read from the footboard. • Two persons are required to measure recumbent length. as shown below .With the child in the supine position (lying on his or her back), one person holds the child’s head against the backboard, with the crown securely against the headboard and with the Frank- fort plane perpendicular to the backboard. 2 • This person also keeps the long axis of the child’s body aligned with the center line of the backboard, the child’s shoulders and buttocks securely touching the backboard, and the shoulders and hips at right angles to the long axis of the body. • The other person keeps the child’s legs straight and against the backboard, slides the footboard against the bottom of the feet (without shoes or socks) with the toes pointing upward, and reads the measurement. The footboard should be pressed firmly enough to compress the soft tissues of the soles but without diminishing the vertebral column length. • Length should be recorded to the nearest 0.1 cm or in., using a consistent unit over • repeated measurements. Gentle restraint is often required to keep a squirming infant properly positioned during measuring. When this is not possible, the best estimate should be recorded with a notation of the circumstances. Stature • Stature, or standing height, can be measured for subjects 2 to 3 years of age and older who are cooperative and able to stand without assistance. Stature can be measured in several ways. • The simplest is to fasten a measuring stick or nonstretchable tape measure to a flat, vertical surface (for example, a wall) and use a right-angle headboard for reading the measurement, If a wall is used, it should not have a thick baseboard, and the subject should not stand on carpet, which could affect the accuracy of measurements. • Using the moveable rod on a platform scale is not recommended because it often lacks rigidity, the headboard is not always correctly aligned, there is no rigid surface against which to position the body, and the platform height will vary depending on the subject’s weight. Another approach is to use a 3 stadiometer, such as the Harpenden stadiometer or one manufactured by Seca Corporation or Measurement Concepts. • When being measured with the stadiometer, the subject should be barefoot and wear minimal clothing to facilitate correct positioning of the body. The subject should stand with heels together, arms to the side, legs straight, shoulders relaxed, and head in the Frankfort horizontal plane (“look straight ahead”). Heels, buttocks, scapulae (shoulder blades), and back of the head should, if possible, be against the vertical surface of the stadiometer. • Some people may not be able to touch all four points against the stadiometer because of obesity, protruding buttocks, or curvature of the spine. Rather than creating an embarrassing situation by trying to force a subject into • a physically impossible position, have the subject touch two or three of the four points to the vertical surface of the stadiometer or estimate height from knee height. • Just before the measurement is taken, the subject should inhale deeply, hold the breath, and maintain an erect posture (“stand up tall”) while the headboard is lowered on the highest point of the head with enough pressure to compress the hair). • The measurement should be read to the nearest 0.1 cm or in. and with the eye level with the headboard to avoid errors caused by parallax, which is a difference in the apparent reading of a measurement scale. Nonambulatory Persons • In nonambulatory persons (those unable to walk) or those who have such severe spinal curvature that measurement of height would be inaccurate, stature can be estimated from knee height. 4 Head Circumference • Head circumference measurement is an important screening procedure to detect abnormalities of head and brain growth, especially in the first year of life. Although these conditions may or may not be related to nutritional factors, discussion of head circumference measurement is included here for convenience. • Head circumference increases rapidly during the first 12 months of life but, by 36 months, growth is much slower,’0 Therefore, it is recommended that head circumference be measured routinely on infants and young children up to age 36 months. • Head circumference is most easily measured when the infant or child is sitting on the lap of the caregiver, although older children can be measured when they are standing. • A flexible. nonstretchable measuring tape is required. Objects such as pins should he removed from the hair. As shown below, the lower edge of the tape should be positioned just above the eyebrows, above not over) the ears, and around the back of the head, so that the maximum circumference is measured. • The tape should be in the same plane on both sides of the head and pulled snug to compress the hair. The measurement is read to the nearest 0.1 cm or in. and written in the infant’s file. Reliability of the measurement should be verified with a second reading. MEASURING WEIGHT One of the most important measurements in nutritional assessment is body weight. Weight is an important variable in equations predicting caloric expenditure and in indices of body composition.” 5 • Body weights should be obtained using an electronic scale or a balance-beam scale • Compared with balance beam scales, electronic scales tend to be lighter in weight, somewhat more portable, and faster and easier to use. They provide easy-to-read digital output in either metric or English units and, when properly calibrated, are highly accurate • Errors are commonly made in reading scale, dials, and rulers. The large. easily read digital output from electronic scales can help reduce this error. • Digital scales can record a subject’s weight quickly. This can be an advantage in weighing infants, who tend to resist lying still for very long. • Scales should be placed on a flat, hard surface that will allow them to sit securely without rocking or tipping. The zero weight on the scale’s horizontal beam should be checked periodically and after the scale has been moved. • On balance beam scales this can be done by sliding the main and fractional weights to their respective zero positions and adjusting the zeroing weight until the beam balances at zero. Two or three times a year the accuracy of the scales should be further assured by using standard weights or by a professional dealer. • Because spring-type bathroom scales may not provide the required accuracy after repeated use, they are not recommended. 6 • Balance-beam scales with wheels that are moved from one location to another are not recommended either because scales must be recalibrated every time they are moved • Infants • Infants should be weighed on a pan-type pediatric electronic or balance-beam scale that is accurate to within 10 g (0.01 kg) or 0.5 OZ. Any cushion (for example, either a towel or diaper) used in the pan should be in place when the zero adjustments are made on the scale or its weight should be subtracted from the infant’s weight.. • Whatever practice is used, it must be uniformly followed and noted in the infant’s file. Infants can be weighed nude, or the weight of the infant’s diaper can be weighed nude, or the weight of the infant’s diaper can be subtracted from the infant’s weight. The infant should be set lying down in the middle of the pan. • The average of two or three weightings is recorded numerically in the infant’s file to the nearest 10 g (0.01 kg) or .5 oz and then is plotted on the growth chart in the presence of the subject’s caregiver. If, on comparison with previous data, the current values appear unusual, the measurements should be repeated. • Excessive infant movement can make it difficult to obtain an accurate weight, in which case the weighing can be deferred until later in the examination. When too active to weigh on a baby scale, an infant can be weighed on a platform scale while being held by an adult with the weight derived by difference. 7 • Children and Adults • Children and adults who can stand without assistance are weighed on a platform electronic or balance-beam scale that is accurate to 100 g (0.1 kg) or .25 lb. The subject should stand still in the middle of the scale’s platform without touching anything and with the body weight equally distributed on both feet. • The weight should be read to the nearest 100 g (0.1 kg) or .25 lb and recorded. Two measurements taken in immediate succession should agree to within 100 g (0.1 kg) or .25 lb.’ The weight of children then can be plotted on their growth charts. • Ideally, children and adults should be weighed after voiding and dressed in an examination gown of known weight or in light underclothing with the scales placed where adequate privacy is provided. Should the weight of clothing be subtracted from the subject’s weight? It depends on the purpose for which measurements are obtained and how accurate they need to be. • In settings requiring a high degree of accuracy, subjects can be clothed in an examination gown of known weight for which consideration can be easily made. In situations having somewhat less stringent requirements, a reasonable estimate of clothing weight can be subtracted from a subject’s weight. Nonambulatory Persons • Persons who cannot stand unassisted on a scale can be weighed in a bed scale or chair scale. The subject to be weighed in the bed 8 scale is comfortably positioned in the weighing sling, which then is gently raised until the subject is suspended off the bed. In a chair scale, the subject sits upright in the center of the chair while leaning against the backrest • Using either method, once the subject is still, weight can be read and recorded to the nearest 100 g (0.1 kg) or .25 lb. Reliability of the measurement can be verified with a second reading, which should agree to within 100 g or ¼ lb.’ • SKINFOlD MEASUREMENTS • The most widely used method of indirectly estimating percent body fat in clinical settings is to measure skinfolds—the thickness of a double fold of skin and compressed subcutaneous adipose tissue . • Although more accurate methods for assessing percent body fat exist, SKINFOlD measurement has these advantages: the equipment needed is inexpensive and requires little space measurements are easily and quickly obtained; and, when correctly done, skinfold measurement provides estimates of body composition that correlate well with those derived from hydrostatic weighing. the most widely used laboratory method for determining body composition. • Measurement Technique • Proper measurement of skinfolds requires careful attention to site selection and strict adherence to the following protocol, which is 9 standard among researchers who developed the prediction equations for determining fatness from skinfold measurements. • 1-Most North American investigators (including those conducting large national surveys rum which reference data are derived) take skinfold measurements on the right side of the body. European investigators typically perform measurements on the left side. From a practical standpoint, it matters little on which side measurements are taken. • 2. As a general rule, those with little experience iii skinfold measurement should mark the site to be measured once it has been carefully identified . A flexible nonstretchable tape measure can be used to locate midpoints on the body. • 3. The skinfold should be firmly grasped by the thumb and index finger of the left hand about I cm or 0.5 in. proximal to the skinfold site and pulled away from the body. This is usually easy with thin people, but it may be difficult with the obese and may be somewhat uncomfortable. • 4. The caliper is held in the right hand perpendicular to the long axis of the skinfold and with the calipers dial facing up and easily readable. The caliper tips • should be placed on the site and should be about 1 cm or .5 in. distal to the fingers holding the skinfold . • 5. The caliper should not be placed too deeply into the skinfold or too close to the tip of the skinfold. The measurer should try to visualize where a true double fold of skin thickness is and place the 10 caliper tips there. It is a good practice to position the caliper arms one at a time on the skinfold. • 6. The dial is read approximately 4 seconds after the pressure from the measurer’s hand has been released on the lever arm of the caliper. If caliper tips exert force for longer than 4 seconds, the reading will gradually become smaller as fluids are forced from the compressed tissues. • 7. A minimum of two measurements should be taken at each site. Measurements should be at least 15 seconds apart to allow the skinfold site to return to normal. If consecutive measurements vary by more than 1 mm, more should be taken until there is consistency. • 8- Measurements should not be taken immediately after exercise or when the person being measured is overheated because the shift in body fluid to the skin will inflate normal skinfold size. • 9-. It takes practice to consistently grasp skinfolds at the same location every time. Accuracy can be tested by having several technicians take the same measurements and comparing results. It may take up to 50 practice sessions to become proficient in measuring skinfolds. • Several types of skinfold calipers are available). The Lange skinfold caliper is most popular among U.S. Several less expensive plastic calipers are available, such as the Slim Guide and the Fat-Control Caliper. • Some of the plastic calipers have been shown to give results comparable to the more expensive calipers. 11